Currently, there is an ambiguous attitude towards vaccinations in society. People refuse vaccination for various reasons. They are contraindicated for some, some think they are contraindicated for them, some refuse for reasons of principle, and some believe that vaccinations are a much greater evil than diseases. I want to emphasize that I do not support these points of view, and I believe that vaccinations are necessary. Therefore, in this article I would like to answer the most frequently asked questions about carrying out or not carrying out preventive vaccination of children.
What types of vaccines are there?
- Live vaccines. They contain a weakened living microorganism. They are able to multiply in the body and cause the vaccination process, forming immunity.
- Inactivated (killed) vaccines. They contain a killed whole microorganism; they are killed by physical or chemical methods. Such vaccines are reactogenic and are rarely used.
- Chemical vaccines. Contain components of the cell wall or other parts of the pathogen.
- Anatoxins. Vaccines containing an inactivated toxin (poison) produced by bacteria. As a result of this treatment, toxic properties are lost, but immunogenic properties remain.
- Recombinant vaccines. Vaccines obtained by genetic engineering. The essence of the method: the genes of a virulent microorganism, responsible for the synthesis of protective antigens, are inserted into the genome of a harmless microorganism, which, when cultivated, produces and accumulates the corresponding antigen.
- Synthetic vaccines are artificially created antigenic determinants of microorganisms.
- Associated vaccines. Vaccines of various types containing several components.
Almost everything about vaccination and revaccination
If new strains infect vaccinated people, is it useless to get vaccinated? Israel and the UK have vaccinated their populations, but the incidence is still rising.
No, it's not useless. In Israel, by June 1, 2021, 80% of the adult population
, or 60% of the population, had been vaccinated.
Among older people, 90% have been vaccinated. by June 1, 75.2% of people over 18 years of age had received at least one dose of the vaccine, and 49.5%
had received two doses.
On June 1, 16.9 million people received at least one dose, 12.8 million received two doses, or about 11%
of the adult population.
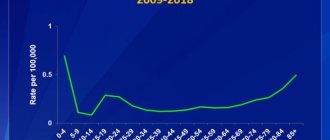
We see in the figure how the next wave caused by the “Indian” delta strain occurs in these three countries. The red line shows the number of new cases per day, the white line shows the number of deaths from COVID-19, and the green line shows the pace of vaccinations.
By: by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU), data as of 07/02/2021
In Israel, the incidence has increased from dozens of cases per day to 200–300 - still an order of magnitude less than in Moscow alone, which means that the transmission of the virus has been suppressed. The daily number of deaths is not growing at all. In the UK there is a fairly sharp increase in new cases, but there are no more deaths - people get sick mildly. In Russia, the situation is different: the number of new cases has grown rapidly, and a record has been set for the number of deaths.
But vaccinated people still get sick, I know such cases!
They get sick, but much easier and less often. Is, which analyzed approximately 14,000 cases of COVID-19 caused by the delta variant in the UK, including 122 hospitalizations, from April 12 to June 4. After two doses, the Pfizer vaccine was 88% protective against delta COVID (that is, the number of people who were expected to get sick but didn't because they were vaccinated fell by 88%). For the AstraZeneca vaccine, the result is more modest - 67%. The level of protection against severe cases requiring hospitalization is virtually the same as for the alpha, that is, the “UK strain”: 96% for Pfizer, 92% for AstraZeneca.
Let us remind you that the WHO and the US FDA consider the vaccine effectiveness to be at least 50% acceptable. And now, after the records of mRNA vaccines and Sputnik V, it seems to us that 67% is not enough.
Sputnik appears to be no less effective than the AstraZeneca vaccine. Details about the share of those who received two doses of the vaccine among those hospitalized (the share is very small) can be seen on Facebook of the head physician of Moscow City Clinical Hospital No. 40. Data is updated regularly. An important clarification about two doses: immunity is not formed instantly after the first injection. Three weeks after the second, you can already consider yourself protected.
So how long does immunity from COVID-19 last after vaccination? Alexander Ginzburg that he is a lifelong candidate, now the Ministry of Health in its guidelines for vaccination states that the concentration of antibodies drops after six months or a year.
One does not contradict the other. The immune response after illness or vaccination includes several components. Antibodies in the blood are a humoral response
.
B lymphocytes begin to actively multiply, producing antibodies against certain sections of coronavirus antigen proteins—such sections are called epitopes. When the virus subsequently appears in the body, these antibodies will bind to viral particles and thereby contribute to its destruction. Neutralizing antibodies
are especially important - against those parts of the S-protein that forms the “crown” spikes that are necessary for binding to the cellular receptor. They directly prevent the virus from entering the cell. Not all antibodies to the S protein are neutralizing, we will discuss this later.
a T-cell response develops
for viral antigens. Killer T cells, also known as cytotoxic T lymphocytes (they are also called CD8+ T cells, although there is a small population of killer T cells with the CD4 marker) destroy cells infected with the virus. Helper T cells (CD4+ T cells) promote the activation of B lymphocytes, killer T cells, and other cells of the immune system.
Antibodies against coronavirus are an important indicator of the immune response. If there are a lot of antibodies in the blood, a repeat infection is highly likely to be asymptomatic, and the immune system will quickly deal with the virus.
Indeed, the concentration of antibodies in the blood decreases over time: in different people at different rates, but it is now clear that within six months to a year the decrease will become noticeable. And this is good: like Konstantin Severinov, if the blood maintained a high concentration of antibodies to all the antigens that we encountered, our blood would look like a gel. However, a decrease in antibody titer does not mean that a person’s immunity has disappeared. There are memory B cells - B lymphocytes that produce antibodies against the coronavirus, which are sent “in reserve”, but can be mobilized in the event of a new encounter with the coronavirus. There are T cells that will not stop the initial infection, but will quickly clear the body of infected cells. (Memory T cells are also produced.) Therefore, a person with a low antibody titer is much more likely to have a mild illness than someone who has not previously been infected or vaccinated.
It is necessary to distinguish between sterilizing immunity
, in which the virus does not multiply in the body, but is destroyed immediately after entering the respiratory tract;
protection from the symptoms
of the disease (the virus can enter the body, but will soon be destroyed and will not cause illness, but a person may be infectious for some time);
and finally, protection from severe disease
and death. We have not yet seen a vaccine that would provide sterilizing immunity against coronavirus. But protection against severe forms is also important. If COVID-19 always had a mild form, it would not be able to ruin the lives of humanity.
Do commercial tests show neutralizing antibodies?
Commercial test systems most often detect antibodies against the coronavirus S protein or its fragments (sometimes against other proteins). Directly determining the titer of neutralizing antibodies is too difficult for mass tests: you need to look at how human blood serum prevents the virus from entering cells. And for this you need a virus or at least a pseudovirus with coronavirus proteins, a cell culture... It is much easier to find out how many antibodies in human blood serum bind to purified coronavirus proteins. Not all such antibodies are neutralizing, but, as a rule, if there are many antibodies to the S protein, then there are many neutralizing antibodies.
What about new strains? Why don't they help the immune response against older strains?
The virus has spread unprecedentedly widely, it is multiplying and mutating. Among the mutations, there are those that change the structure of epitopes, and then the antibodies in the blood of those who have been ill and vaccinated are less able to recognize the changed virus.
This does not mean that antibodies do not recognize them at all. There are more epitopes in viral proteins than can be affected by mutations in a particular strain, so escape is not complete. Of the many known lineages of the virus, only a very few have been considered “of concern.”
A recent example from Moderna, which is testing the effectiveness of its vaccine. To neutralize the "British" B.1.1.7, or alpha, you only need 1.2 times more neutralizing antibodies. For A.VOI.V2, first discovered in Angola, and one of the variants of the “South African” B.1.351 - 8.0 and 8.4 times, respectively, and for the terrible B.1.617.2 (delta) - 2.1 times. This means that people with high levels of antibodies against the old strain are more likely not to get sick with the new one.
Happiness is not only in antibodies. The good news is that T-cell immunity against new strains declines much less noticeably. T cells do not recognize the same epitopes as neutralizing antibodies, and these epitopes change more slowly in the virus.
In the future, could a strain emerge that hacks the immune defense more effectively than those already known?
Experts are trying to assess the likelihood of such a sad event, but there are too many factors at play. There is a known way to reduce the likelihood: reduce the virus population as much and quickly as possible. And to do this, vaccinate the population. And not only in high-income countries, but also in sub-Saharan Africa. We just didn't have enough Angolan strains.
What happens during revaccination?
Revaccination simulates a second encounter with the pathogen, which will “awaken” memory B cells and other components of the immune system. Only without the risk of getting sick, because not a single vaccine contains live coronavirus. According to all available data, a repeated dose of the vaccine or a second encounter with the virus leads to a sharp rise in antibody titer.
Why do they say that you cannot be vaccinated again with adenovirus vaccines, for example, Sputnik V?
Unlike many other vaccine concerns, this one makes sense. The vaccinated person may have antibodies to the adenoviral vector, which delivers the coronavirus S-protein gene into the body. If the immune system deals with the vector before the S-protein begins to be produced, this will reduce the effectiveness of vaccination. The appearance of antibodies to adenoviral vectors was observed in clinical trials of Sputnik V (Gam-COVID-Vac). For this same reason, our developers took two different adenoviruses for the first and second doses of the vaccine, serotypes 26 and 5.
However, developers of other two-dose adenovirus vaccines used the same vector, and the second dose worked. Immunity against natural adenoviruses from which the vectors were derived does not appear to be particularly robust.
At the end of June, AstraZeneca began testing a vaccine adapted against the “South African” strain of coronavirus (B.1.351, or beta). Some of the volunteers were vaccinated with the “old” AstraZeneca vaccine no later than three months ago. The fact that both vaccines contain the same vector based on chimpanzee adenovirus does not bother the organizers. Thus, practice seems to have refuted these fears.
How high should the antibody concentration be to avoid getting sick? The Ministry of Health deliberately says that this is unknown, because it really wants to vaccinate everyone?
There is no magic number about which you can say: “If you have so many antibodies, you won’t get sick.” And because the immune system is complex, and because of new strains, and for a number of other reasons.
“Currently there is no validated marker (specific protective antibody level). Work to develop such a parameter is at the research stage and has not yet been accepted, including by WHO,” says the Temporary Guidelines of the Ministry of Health. And it is true.
Yes, the concentrations of antibodies to S-protein, which are determined in diagnostic centers, correlate with titers of neutralizing antibodies, but determining which numbers on the test form indicate reliable protection is not easy. Commercial test systems provide results in conventional units, which are different for each manufacturer. WHO is working to standardize test systems: serum samples with which the manufacturer can correlate its arbitrary units and international units of neutralizing and binding activity of antibodies. Once all manufacturers have done this, it remains to be seen exactly what level of neutralizing antibodies is sufficient for protection. (Upd: Roszdravnadzor has published conversion factors, which will at least make it possible to compare the results of various tests with each other.)
There is an approximate way: go from the average level of neutralizing antibodies in those who have recovered from the disease. This indicator is often used as a kind of conditional standard; for example, you can compare the average level of antibodies in vaccinated people with it and say whether the vaccine is good or bad. There are articles where the results of commercial tests are compared with titers of neutralizing antibodies (for example, this one). From them you can find out what test value corresponds to the average titer in those who have recovered (for example, for DiaSorin S1/S2 IgG, a result of 45.1 FU/ml was obtained for 62 recovered patients). that for 50% protection against SARS-CoV-2 infection, the level of neutralizing antibodies in a person should be about 20% of the average level of neutralizing antibodies in those who have recovered from the disease, or about . In fact, the confidence intervals there are quite wide, but this way you can make a rough estimate. But since the strain in Moscow is delta, and all these calculations were done before, we multiply the minimum protective level by 2 or, to be sure, by 3...
In general, these are educational exercises, but the exact level of antibodies that guarantee protection against COVID-19 cannot be calculated in this way. The maximum you can count on is that you will understand whether you have “a lot” of antibodies or “a little.” As disgusting as it is to admit, the Ministry of Health is right: it is better to focus on the time that has passed since vaccination or illness. But a negative result—the antibody level is below the threshold or close to it—is informative. In this case, you need to get vaccinated.
Is there a level of antibodies that protects against the delta strain? The answer to this question is now being sought by the “people’s testers,” an initiative group that studied the effectiveness of the Sputnik V vaccine.
What about the side effects of vaccines?
The short answer is that they are incomparably less dangerous than the complications of COVID-19. Without going into detail, you can look at the percentage of those who die as a result of SARS-CoV-2 infection, and it is also useful to remember what this applies to you and your contacts, and keep these results in mind while we collect data on harmfulness of vaccines.
It is necessary to compare the complications from the vaccine with the complications from the disease. The option “not to get vaccinated and not get sick” is no longer available for any of us. Every person on Earth will receive antibodies to SARS-CoV-2, either after vaccination or after illness.
Side effects of vaccines are described in sufficient detail in articles that present the results of clinical trials (CTs). We are mainly talking about high fever, headache, pain at the injection site, etc.
The story of suspected transverse myelitis in a British patient vaccinated with AstraZeneca, due to which the vaccine trial was stopped in the fall, apparently did not continue: the connection has not been proven. The incidence of thromboembolic events following AstraZeneca continues to be discussed; Perhaps their frequency increases after other vaccines. The cases are truly rare, tens of millions (unlike complications associated with blood clotting after COVID-19: preventive anticoagulants are prescribed after it for a reason). For those to whom this happened, of course, it is not easier because the cases are rare. The right approach is to focus on if a rare event occurs in our area.
They write about rare (again, tens of millions) cases of inflammation of the heart muscle, or myocarditis, in young patients after mRNA vaccines (,). The order to avoid physical activity after vaccination is given for a reason. At the same time, up to 60% of people after severe COVID-19 have heart damage in one way or another, and in almost 1% of athletes who have had mild COVID-19, MRI reveals myocarditis, so vaccination remains a safer choice in this regard.
But the long-term effects of vaccination have not been studied!
Yes. They cannot be studied because we do not have people who were vaccinated earlier than the spring of 2021. But the long-term effects of COVID-19 have also not yet been studied, and the available evidence suggests that they are varied, unpleasant and, apparently, not limited to harm to the lungs and circulatory system.
They say the vaccines have not been tested enough. Usually they are tested for decades, but these ones were done in less than a year. Is this reliable?
Yes, usually the development of a vaccine takes 10–15 years, but when vaccines against coronavirus infection were needed, it took a year. They saved time. Firstly, they used “homemade preparations”: platforms on which they had already tried to make vaccines against other diseases, ideally those that had already entered clinical trials. This allowed us to shorten the preclinical phase (testing on animals). Secondly, phases 1, 2 and 3 of clinical trials did not occur one after another, but “overlapping”: as soon as preliminary results showed that the goal was likely to be achieved, the next phase was launched. Moreover, the production launch began simultaneously with the clinical trials.
It was a risk, primarily financial. “In peacetime,” no one starts the expensive third phase of a CI involving tens of thousands of people until the previous ones are completed. No normal company launches production of a drug that has not completed a clinical trial. All in all, it was a case of money buying time.
The risk is real: some of the developments ended in failure. An anecdotal failure occurred with a promising vaccine from the University of Queensland in Australia, which launched at the same time as Moderna. Some of those vaccinated had Who would want to go through this, even for protection against COVID-19? The German vaccine CureVac may not reach 50% effectiveness. When a clinical trial of the AstraZeneca vaccine was stopped due to a participant’s illness, they could have frozen her too if a cause-and-effect relationship had been confirmed.
Finally, it was possible to save a lot of time on paperwork - registering vaccines with regulatory authorities. Review of documents submitted for registration of a medical product can take up to two years. Now they have done it in a matter of months: the regulator began to receive data on clinical trials even before the end of the third phase, and since the whole world was looking at it with hope, it reduced the ceremonies to a minimum.
Special conversation about Russian vaccines. For example, what was the meaning, other than political, of the solemn “world’s first” registration of the vaccine at the NICEM. N.F. Gamaleya not only until the end of phase 3, but even before the publication of the results of phase 1-2? (Other leading vaccines passed their main milestones no later than the Russian one, see. .
) The results turned out to be quite worthy, but mistrust arose, and the consequences are still affecting us. The results of the clinical trial of the EpiVacCorona vaccine, which has many questions, have not yet been published, and at the same time it is already being transported to vaccination points. The results of the CoviVac clinical trial have not been published, but we began to expect them relatively recently.
What reactions are currently occurring to vaccines?
The number of adverse reactions is minimal, since modern vaccines usually consist of 95% antigen. Redness and induration rarely occur at the site of vaccine administration. In rare cases, a slight increase in body temperature may occur.
In conclusion, I would like to note that only his parents can decide whether to vaccinate a child or not. And no one has the right to force them.
But it is worth thinking about the fact that if complications or adverse reactions from vaccines occur, they are still much less dangerous than the diseases for which these vaccinations were given.
Basics of vaccination
Today, talking about vaccination is both easy and difficult at the same time, notes Tatyana Romanenko.
“This is a method of individual or mass protection of the population from infectious diseases by creating or enhancing artificial immunity using vaccines. Vaccination is the most effective and cost-effective means of protection against infectious diseases known to modern medicine,” notes the therapist.
Life-saving vaccine. How are vaccines developed today? More details
Its main principle, notes Tatyana Romanenko, is the introduction into the body of a vaccinated “weakened or killed” pathogen (viral or bacterial agent) or an artificially synthesized protein/antigen that is identical to the protein/antigen of the infectious agent in order to stimulate the production of antibodies to combat the pathogen. In this case, vaccination can be either single or multiple. The frequency indicates how many times a person needs to receive the vaccine to develop lasting immunity.
Vaccinations are given against various pathogens. These include a variety of viruses - COVID, causative agents of measles, rubella, mumps, polio, hepatitis B; bacteria - causative agents of tuberculosis, diphtheria, whooping cough, tetanus, hemophilus influenzae. “As a result, antibodies are formed, which means that protection has been formed. And another question arises - what next? Here it is worth understanding that over time, the “cartridges” (antibodies) run out. And this should not surprise anyone. And to solve this problem, revaccination exists,” says Tatyana Romanenko.
And it is worth fully observing all schedules, since the more people are immune to a particular disease, the less likely it is for others who are not immunized to get sick, and the less the risk of developing an epidemic. This means that compliance with the vaccination and revaccination schedule is caring for loved ones. “To maintain epidemic well-being, vaccination coverage of at least 95% of the population is required,” the therapist emphasizes.
Contraindications
Vaccinations should not be given if the patient:
- serious allergic reactions to previous administrations of this vaccine have been observed,
- are allergic to vaccine components (for example, chicken egg white),
- the patient is in the acute phase of the disease,
- there are serious chronic diseases, the immune system is depressed.
Pregnancy is often the reason to refuse vaccination. Details about all contraindications can be found in the instructions for use for each drug separately. Before getting vaccinated, consult your doctor.
Misdirected immunity during vaccination - an example of RSV-lot100
In the early 1960s, the first RSV vaccine was created and tested on infants and young children. To do this, the virus was inactivated with formalin and an aluminum-based adjuvant was added, and the vaccine was administered to children aged 1 to 7 years in two or three intramuscular doses with an interval of 1-3 months. The vaccine was not only able to provide protection against disease following wild-type RSV infection, but also induced an exaggerated pathological response to wild-type RSV infection in vaccinated children. Many children were hospitalized with diseases of the lower respiratory tract. In one study, the rate of RSV-related hospitalization in vaccine recipients was exactly 80%, compared with 5% in controls. Tragically, two vaccinated children died from RSV infection.
A good immune response to a vaccine is usually determined by measuring antibodies. The majority of children vaccinated with RSV-lot100 seroconverted after vaccination with high titers against RSV-F protein. The problem with the vaccine was thus not the lack of induction of immunity, but the induction of “wrong” “false” immunity. To understand and avoid such pathological immune reactions, it is necessary to have a clear understanding of the role of specific B and T cell responses in the control of viral infections and immunologically mediated pathology. In particular, the following questions should be answered:
- What role does B cell play? T-cell immunity in protection against disease?
- What role do CD4+- vs. CD8+ T-cells, what role do Th1- vs. Th2 cells?
- What is the role of local vs. systemic T-cell immunity, virus-specific IgA vs. IgG?
Some of these immunological aspects will be presented below. Ultimately, they were studied individually for each virus, since each virus-host interaction is different from each other. These considerations can best be illustrated with a specific example. For this purpose and in further presentation, we must use RSV infection.
Vaccinations according to epidemiological indications
Vaccinations against tick-borne encephalitis. Conducted for populations living in areas where this disease is endemic.
Vaccinations against meningococcal infection, mumps, chickenpox, typhoid fever, cholera.
In endemic areas, the population or individual risk groups can also be vaccinated against tularemia, leptospirosis, plague, brucellosis, rabies, anthrax, Q fever, yellow fever (when traveling to countries where this infection is registered), says the therapist.
Flu, rubella, tetanus. What should adults be vaccinated against? More details
Attenuated live vaccine as an ideal vaccine?
The goal of inducing balanced immunity against RSV or other viruses is likely to be achieved by local vaccination with an attenuated live vaccine. The advantages are the physiological route of immunization with the activation of local and systemic immunity, as well as the optimal balance between B-cell and T-cell immunity.
The difficulty in creating such a vaccine lies in the difficulty of selecting the correct degree of attenuation. If you attenuate too much, no sufficient protection will be achieved. If the attenuation is too weak, you should expect side effects typical of an infection, such as, for example, with RSV, blockage of the airways with refusal to drink or sleep disturbances. Also, rare incidents such as the incidence of sudden infant death should be carefully analyzed in vaccine studies, as has been shown by the increased incidence of intussusception following vaccination with locally administered live rotavirus vaccine. In the current development of a vaccine against RSV, the issue of correct attenuation continues to remain the main problem, even if in the meantime it has become possible to manipulate the RSV genome and quite purposefully induce attenuation mutations. A number of promising candidate vaccines still require a long period of experimental work before their use in adults, children, and finally before testing on seronegative infants (Fig. 7). So far, however, none of the viral isolates show the correct size attenuation. Even if attenuated live vaccines seem to be an ideal vaccination strategy from an immunological point of view, numerous problems still need to be solved in practice.
What actions should parents take after vaccination? Are there any restrictions?
I repeat, vaccination is a completely standard procedure, so you should not put your child to bed and be “overprotective” of him. The family can live their normal lives, but, of course, remember that the child was vaccinated, and maybe be a little more attentive to the child.
When administering DPT and other serious vaccines in the next three days, try to adhere to a more or less gentle regimen for the child, that is, it is advisable to avoid unnecessary visits, limit contacts and the overall burden on the child. At this time, the baby is shown a calm home regime. Walking is not prohibited. Just try to cover the grafting site with clothing to prevent dirt from getting on it. And, of course, the walk should be of a reasonable length.
It is also recommended not to experiment with nutrition, that is, not to introduce new foods into the child’s diet, in the period a week before vaccination and a week after. If a child is prone to allergic reactions, during this period he should receive food that excludes those foods that can cause allergies.
If your child has had an injection (and almost all vaccines are injectable), try not to bathe him or her for a day after the shot. The next day, you can take a bath as usual, again, if the child does not have a temperature reaction.
After vaccination against polio, which is dripped into the mouth, it is recommended to limit food and drink for an hour, since the live polio vaccine can be washed off from the mucous membranes and not give the expected effect. This restriction does not apply to other vaccines that are administered by injection.
Thus, as you can see, the recommendations are the simplest. Strict restrictions are introduced in special cases related to vaccination of groups of children with severe chronic diseases, severe allergies, and so on.
The sanitary rules establish a recommendation regarding the post-vaccination period, according to which, after vaccination, a child should stay in a medical facility for 20-30 minutes. It is during this time period that the first manifestation of a possible allergic reaction is most likely. However, such situations in children, fortunately, are extremely rare. Parents who are concerned about the child's condition after vaccination can always stay and spend this time under the supervision of a doctor in a medical facility. If a child is prone to an allergic reaction, this condition must be met.
And one last thing. Before going for vaccination, it is advisable to have an antipyretic drug at home in case the child develops a fever in the evening. For babies under 1 year of age, it is better to take suppositories; for older children, a tablet preparation or in the form of syrup is suitable. The threshold at which it is necessary to reduce the temperature is different for each child. Parents can determine for themselves based on the child’s condition whether he needs to be given an antipyretic,
Can multiple vaccines be administered at the same time?
Mothers of infants worry that vaccinations “kill” their own immunity and can cause harm if administered simultaneously. In reality, every person encounters tens and hundreds of bacteria and viruses every day, and his immune system successfully copes with them.
Two-, three-, four-, and five-component vaccines are well tolerated by children and help develop immunity by the time the kids attend preschool institutions, clubs or sections. You can get complete information about the procedure for administering drugs from your pediatrician.