This message (material) was created and (or) distributed by a foreign media outlet performing the functions of a foreign agent, and (or) a Russian legal entity performing the functions of a foreign agent.
Sign the petition demanding the repeal of the law on foreign agents!
The whole world is looking forward to the end of the “non-working days”, the period of “social distancing” or “lockdown” - depending on how antiviral measures are called in a particular country. However, Mark Lipsitch, a professor at the Department of Epidemiology at Harvard University, warns that the spread of the disease will not stop until there are enough people in the population vulnerable to coronavirus. Simply put, the epidemic will not stop until most of us get sick—or until a coronavirus vaccine becomes available. But why is there still no vaccine? Let's figure it out.
All Meduza materials about coronavirus are open for distribution under a Creative Commons CC BY license. You can reprint them! Photos are not licensed.
As of April 30, 2021, World Health Organization (WHO) staff are aware of 102 anti-coronavirus vaccine candidates, with eight vaccines already undergoing clinical trials on healthy people. However, the real number of vaccine candidates may be higher: not all companies that are trying to create a “magic pill” against COVID-19 are on the WHO list.
The principle of action of already existing and still being developed vaccines is based on several ways to induce an immune response in the body, and each method has its own advantages and disadvantages. It's impossible to predict which type of vaccine will work best before human clinical trials begin, so drug companies are forced to fly almost blindly, trying different methods. But maybe this is for the best: if one type of vaccine turns out to be ineffective or unsafe, there is always a chance that another type of vaccine will work better.
Chapter 1
Viral vaccines
Vaccines based on weakened virus
What is this? A vaccine that contains the SARS-CoV-2 virus, which has been very weakened (in other words, attenuated) in the laboratory. This type of vaccine has been known since the 1950s: the principle behind the measles, mumps, rubella (MMR) and chickenpox vaccines.
What is the mechanism of action? To create a vaccine, laboratory workers use a virus that is successively infected in laboratory animals. The fact is that viruses adapt to the host in whose body they find themselves. If you forcibly “relocate” a human virus into an animal cell culture, the virus will begin to mutate. Thus, after each cycle of infection, the virus will adapt better to the new host - and at the same time become less and less dangerous to humans. At the same time, the mutated “animal” virus still remains sufficiently similar to the original “human” one to cause a full-fledged immune response in the vaccinated person. If a vaccinated person becomes infected with the original “wild” virus, his immune system will already be ready to meet and quickly cope with the disease.
What's good about this vaccine? Immunity from this vaccine lasts the longest. In the case of COVID-19, this is especially important, because strong immunity to coronavirus infections is not always formed.
What's the problem with the vaccine? We know very little about how viruses mutate, so the process of creating a live vaccine is largely unpredictable. There is always a chance that a weakened virus will “regain its strength” and “learn” to cause disease again. To prevent this from happening, we have to very carefully study viruses and organize scrupulous clinical trials of the resulting vaccine, which will take several years. If a “live” vaccine can be created, it will have many advantages - but such a drug will not appear any time soon.
Who is working on the vaccine and at what stage is it? The American company Codagenix (developed jointly with the Indian Serum Institute) announced the start of development of a vaccine based on a weakened virus on February 13, 2021. According to WHO, as of April 30, 2021, the vaccine is in the preclinical testing phase - that is, it either has not yet been created or is being tested on laboratory animals.
How are medications tested?
- I was offered to participate in clinical trials. Is it worth agreeing to this?
Inactivated vaccines
What is this? A vaccine that contains inactivated viruses, that is, not capable of infecting cells. This is also an old and proven type of vaccine: the principle underlies vaccinations against polio and whooping cough.
What is the mechanism of action? To create a vaccine, viruses are inactivated - heated, treated with ionizing radiation or disinfectants. Although the proteins of “killed” viruses change shape (that is, denature), their chemical composition remains the same - and the viral particles themselves partially retain their original shape. Dead viruses can also trigger an immune response.
True, such vaccines have two drawbacks. Firstly, such vaccines usually cause too weak an immune response, so substances called “immune response enhancers” - adjuvants - have to be used. The purpose of adjuvants is to help immune cells (B lymphocytes) produce more protective antibody proteins.
Most vaccines use aluminum salts as a universal adjuvant, but vaccines containing aluminum do not help prevent viral infection. Through trial and error, scientists have become convinced that antiviral vaccines can enhance virosome adjuvants. These are “stuffed viruses” in the form of lipid nanoparticles - microscopic droplets of phospholipid fats, onto the surface of which a viral antigen protein is “attached”. Immune cells mistake the dummies for real viruses and react to them more vigorously than to just viral antigen proteins.
Secondly, the “educational material” for the immune system eventually runs out, so the resulting immunity is not as durable as in the case of vaccines based on a weakened virus that can multiply in the body for some time. To maintain immunity, you have to resort to repeated vaccinations.
What's good about this vaccine? Inactivated vaccines are safer than “live” ones - because they do not contain a weakened virus that can mutate.
What's the problem with the vaccine? Most likely, an inactivated SARS-CoV-2 vaccine will cause a weak immune response. For it to work well, it will have to select an effective adjuvant - that is, look for the optimal parameters of the phospholipid virosome droplet. This will require additional time and effort.
Who is working on the vaccine and at what stage is it? According to WHO, as of April 30, 2021, two Chinese developers have achieved the greatest success in creating an inactivated vaccine. Sinopharm is preparing two vaccines at once. The drug, created in collaboration with the Wuhan Institute of Biological Products, is in the first phase of clinical trials - the tolerability of the vaccine is tested on healthy people. The drug, created jointly with the Beijing Institute of Biological Products, is at the very beginning of development - at the stage of regulatory approval.
The most information about the inactivated vaccine is from Sinovac, which is also in the first phase of clinical trials. This company cooperates with the American company Dynavax, which transferred to Sinovac an effective adjuvant that has shown itself well in the hepatitis B vaccine - so it is not surprising that the Chinese developer has taken the lead, because it saves him a lot of time.
On April 19, Sinovac published a preprint - a preliminary version of an article in which they showed that their vaccine works: it stimulates the formation of antibodies against 10 strains of SARS-CoV-2 in mice, rats and rhesus macaques. Although it’s still too early to rejoice - we don’t yet know how the vaccine will perform in humans.
Chapter 2
About new Covid-19 vaccines
An analysis of the results of clinical trials and mass vaccination with the Sputnik V vaccine did not reveal a single case of cerebral venous sinus thrombosis (CVST), this is stated in the official statement of the N.F. Gamaleya Research Center for Epidemiology and Epidemiology, the developer of the first Russian anti-coronavirus vaccine .Each vaccine based on the adenoviral vector platform has its own individual characteristics, and direct comparison between them is incorrect.
Specifically, AstraZeneca's vaccine uses a chimpanzee adenovirus vector to deliver an antigen consisting of the S protein combined with a tissue plasminogen activator leader sequence, the developers said.
The vaccine from Johnson & Johnson uses a human adenovirus serotype 26 vector and full-length S protein, stabilized by introducing mutations. In addition, its production is carried out in the PER.C6 cell line (these are human embryonic retinal cells), which is not widely represented among registered products.
“Sputnik V” is a two-component vaccine that uses adenovirus serotypes 5 and 26. It does not use a fragment of tissue plasminogen activator, and the antigenic insert is an unmodified full-length S-protein. To produce the Sputnik V vaccine, the HEK293 cell line is used, which has long been used for the production of biotechnological products.
Thus, all of the above vaccines based on adenoviral vectors have significant differences in structure and production technology. In this regard, there is no reason to extrapolate the safety data obtained from the use of one vaccine to the safety data of other vaccines.
The highest quality and safety of the Sputnik V vaccine is also ensured by the fact that in the production of Sputnik V, unlike other vaccines, a 4-stage purification technology is used, including two stages of chromatographic purification and two stages of tangential filtration. This technology makes it possible to obtain a highly purified drug, which undergoes mandatory control for the content of residual DNA in the drug, the Gamaleya Center clarifies.
Moreover, adenoviral vectors contain tens of times less nucleic acid compared to the Pfizer and Moderna vaccines (1-2 μg in Sputnik V versus 50 and 100 μg in the Moderna and Pfizer vaccines, respectively).
A study published in The New England Journal of Medicine on April 9, 2021, discusses that a possible trigger for thrombosis in other drugs may be insufficient purification of the drugs, which may result in them containing large amounts of residual DNA. If the target RNA/DNA is not sufficiently purified or if very high doses of the target RNA/DNA are used, other formulations may experience undesirable interaction of the patient's platelet-activating antibodies with elements of the vaccine itself and/or residual DNA/RNA that may form a complex with PF4.
Mikhail Moskvin Kostin discusses vaccines in more detail:
Whole virion inactivated vaccines
Let's start with the “classics”, which dates back to the times of Jenner and Pasteur - whole virion (containing whole virus particles) inactivated or live vaccines, which have proven themselves for centuries in the fight against smallpox, rabies or measles. Everything with such vaccines is simple and clear - a killed (inactivated) or live weakened (attenuated) virus is injected into the patient, after which he becomes mildly ill (live vaccine) or reacts to viral particles (inactivated virus). After this, a person usually develops, to one degree or another, stable humoral (antibodies) and cellular (T-lymphocytes and other cells) specific immunity to this type of virus. The advantages are obvious - everything happens “naturally”. This occurs with the disease itself, but occurring in mild or abortive (interrupted) forms. The immunity is complex and strong, as strong as it can be in relation to a given infectious agent. The disadvantages are a direct continuation of the advantages of the method - people have reactions that are quite comparable to the disease itself, and complications characteristic of the disease itself may arise. Vaccines are “hard”, but during periods of epidemics they are often the most applicable and necessary.
Today, three laboratories have already prepared whole-virion inactivated vaccines for widespread use in China (Sinovac; Beijing Institute of Biological Products/Sinofarm; Wuhan Institute of Biological Products/Sinofarm). In our country, such a vaccine was prepared for widespread use by the M.P. Chumakov Federal Scientific Center for Research and Development of Immunobiological Preparations of the Russian Academy of Sciences. (FGBI FNTSIRIP named after M.P. Chumakov RAS, hereinafter and everywhere “Center named after Chumakov”), traditionally specializing in live and inactivated “classical” vaccines.”
Recombinant vaccines
Relatively innovative vaccines (whose widespread use dates back “only” a couple of decades) are vector vaccines, including those made on the “adenoviral platform.” We need to pay special attention to them, since they include the Sputnik V vaccine, which is already ready for widespread use in Russia. Developed and implemented by the National Research Center for Epidemiology and Microbiology named after honorary academician N. F. Gamaleya of the Ministry of Health of Russia (FGBU N. F. Gamaleya Research Center for Epidemiology and Microbiology of the Ministry of Health of Russia, hereinafter and everywhere else “National Research Center named after Gamaleya”).
To create such vaccines, in particular, a modified DNA-containing human ARVI virus is used - an adenovirus belonging to safe serotypes (immunologically detectable types) 5 and 26 (Ad5, Ad26). These viruses are widespread in various countries (especially serotype 5) and usually cause fleeting seasonal diseases, most often in the form of a runny nose, catarrh of the upper respiratory tract, minor cervical lymphadenitis or intestinal upset (the so-called “summer flu”).
This virus is suitable for use as a “vector”—a carrier that allows delivery into cells of an important DNA sequence necessary for immunization, encoding the proteins of a completely different virus, in this case coronavirus 2 (SARS-CoV-2), which causes COVID-19. The result is a combination that we sometimes called “traveler in a boat” in the laboratory. Where the “boat” is a modified adenovirus, and the “traveler” is a DNA fragment encoding the S-protein of the spike of the viral particle. Which form a “crown” around the shell (nucleocapsid) of the coronavirus. It is to this “corona” that we should receive coronavirus-neutralizing antibodies after immunization. Here is a “hybrid” artificially made from two viruses – adenovirus and coronavirus.
At the same time, for the sake of safety, an important DNA fragment of its genome is removed from the adenovirus, which is responsible for initiating its reproduction inside cells (viruses are intracellular parasites and are themselves incapable of reproduction outside cells). However, such an adenovirus vector retains the ability to initiate in the cells infected by it the production of not only the “boat” of its adenoviral proteins, but also the material of the “traveler”, that is, the S-protein of the coronavirus spike. Each cell infected with such a “hybrid” virus-vector, for example, of the nasal mucosa, does not become a “production shop” for the production of adenovirus, but serves as a small “factory for the production” of the coronavirus S-protein, which is necessary for the development of long-term immunity to it.
Thus, the adenovirus vector enters the body, invades cells, but does not cause their death, but ensures the production of an antigen important for immunization for many days and even weeks. The body recognizes the virus's S protein and gradually produces antibodies to it over approximately 14 to 28 days after immunization. At the same time, fine tuning of cellular immunity occurs. Such immunization usually takes place more calmly and “gently” than when using classical vaccines, and the immunity obtained is usually strong and high-quality.
True, sometimes there are failures, because “where it’s thin, it breaks.” So, if a person has recently been ill with an adenovirus of a given Ad5 or Ad26 type, and he has active immunity against it. In this case, the “boat” will be detected by antibodies and “sunk” even before it has time to deliver the “traveler” to its destination. There may also be a situation when, immediately after vaccination, a person becomes infected with any other adenovirus, the “summer flu” that roams the population. The “wild” adenovirus will “share” the production of the gene missing in our “boat”, and our vector, initially incapable of reproduction, will temporarily become a replicating virus again and will also begin to reproduce in infected cells. In this case, the immune response may be altered, distorted, or unexpectedly enhanced (viral interference). Both situations are possible, but, as many years of practice have established, this usually does not entail the danger of complications. Any vaccination is fraught with risks, but in the case of recombinant vaccines based on adenoviruses, they are minimized. Yes, there are reactions from vaccinations with such vaccines: fever, weakness, etc. at a level that is usually close in severity to seasonal flu vaccines for adults.
Let's move on to the current situation. Four recombinant vaccines are now offered for widespread use in the world:
• American (Janssen Pharmaceutical Companies) based on the Ad26 platform.
• Chinese (CanSino Biological Inc./Beijing Institute of Biotechnology) on the Ad5 platform.
• Russian “Sputnik V” (Gamaleya Center) on two platforms Ad5 and Ad26 at once
• British-Swedish vaccine (University of Oxford/Astra Zeneca), which is not based on human material, but adenoviruses of primates (chimpanzees) were chosen as a “boat” for delivering the “traveler” into cells.
It is clear why the British took primate adenoviruses as a platform. The human immune system has never encountered “Covid” viruses, it cannot recognize them, the “boat” will not be flooded, and with a probability close to 100% it will deliver the “traveler” (the gene encoding the S-protein of the coronavirus) to its destination - into cells epithelium of the mucous membrane, on which there is a marker - the SARS protein, necessary for the introduction of the adenoviral vector into them.
In the case of the Chinese vaccine, the problem is that the “boat” - the Ad5 vector - will be “sunk”, that is, the vaccine is inactivated by the immune system, is very large, since this serotype is very common. For the American vaccine based on Ad26, this probability is much less, but significant. Russian scientists took a special path: since vaccination with vector vaccines is carried out twice (primary and additional “booster”), both platforms were chosen - Ad5 and Ad26, which increases the likelihood of successful immunization, but still does not make it 100%.
It seems that the Swedish-British vaccine in terms of delivery into cells is more reliable than all three others - Russian, Chinese and American, but its “origin from a monkey” makes you think a little: viral material of a different type will enter the human body, which in the event of virus interference or mutation of the virus itself monkeys in the human body can give unexpected results. There are alarming moments in this, although the practice of British scientists has shown that such a platform does not seem to pose a danger to patients. But everything happens for the first time.
However, if I were offered, in the absence of a choice, immunization against coronavirus with one of the four recombinant vaccines described above, I would agree to any of them. Given such a choice, I would choose Sputnik V - both the delivery guarantees are higher than those of the Chinese and Americans, and the material is human, and not taken from our distant relatives from the African forest. So, regarding recombinant vaccines, they are all related to each other, their level of safety is approximately the same, and the fact that from time to time someone starts to say something different about the Sputnik V vaccine is just a consequence of competition or misconceptions, no more. All four of these vaccines are quite reliable.
Now about the next vaccine, in this section, there is only one - EpiVacCorona. Developed, tested and already introduced into civilian circulation by the Federal Budgetary Institution of Science "State Scientific Center of Virology and Biotechnology "Vector"" of the Federal Service for Surveillance in the Sphere of Consumer Rights Protection and Human Well-Being (SSC VB "Vector", hereinafter and everywhere else "Center Vector" ). This vaccine contains only fragments of the coronavirus S protein itself, and does not contain any genetic material from any viruses or cells.
Three fragments of the S-protein of the SARS-CoV-2 virus are “sewn” to a certain protein base and immobilized on aluminum hydroxide particles (acting as an auxiliary stimulus for the development of immunity - an adjuvant). The vaccine is “gentle”, calm, but probably not as strong as the classic or recombinant ones described above, especially in terms of creating cellular immunity. Such “softness” and some one-sidedness of the vaccine in some cases could cause some caution. The fact is that for a number of viral diseases caused by certain viruses (including the related coronavirus (SARS-CoV) of acute pulmonary distress syndrome - “SARS” of 2002-2003 in Southeast Asia). Individuals who were unable to form full-fledged immunity upon first contact with a virus or after the first vaccination against such a virus sometimes experience a syndrome of increased disease upon re-infection or infection after an ineffective vaccination (antibody-dependent enhancement, ADE). A too (mild) vaccination, which only partially protects, could theoretically pose the same danger in the case of coronavirus.
For Covid-19, such a worsening of the course of the disease upon re-infection or after an ineffective vaccination has not yet been reliably shown and even refuted, however, taking into account the relationship of the SARS-CoV viruses and our SARS-CoV-2 virus, one should not relax.
It will be necessary to carefully monitor the situation with the course of Covid-19 in the event that someone suddenly develops the disease shortly after vaccination. We must not let our guard down in this matter. If they ask me today what I would prefer for myself, I would probably choose Sputnik V from the Research Center named after. Gamaleya, although I would also calmly get vaccinated with EpiVacCorona, since I do not consider the risk of ADE significant. “EpiVacCorona” is today recommended by experts for elderly and sick people with allergic diseases as the “mildest” and most gentle vaccination option. Also, it should be noted the special role that EpiVacCorona can play in the future during revaccinations, where its hypothetical disadvantages turn into obvious advantages, which I will discuss separately below.
mRNA vaccines
And finally, the trumpet and triumphant sounding two American vaccines (BioNTech\Fosun Pharma/Pfiser; Moderna\NIAID) based on messenger RNA (messenger RNA, mRNA), encoding the same S-protein of the coronavirus spike, and also, as is the case with recombinant vaccines delivered to the body’s cells in “boats” of lipid nanoparticles.
Vaccines based on mRNA, synthesized on an industrial scale, seem to be very promising, although unknown. They have great advantages over many others in terms of stimulating the immune system without any contact of the human body with viruses. Such a vaccine is also a “traveler in a boat” - a nanoparticle, microvesicle, or “bubble” is usually taken as a “boat”, in which the mRNA encoding the synthesis of only one single protein travels as a “traveler”. The cells into which the mRNA enters are not destroyed, protein production lasts several days, and good cellular and humoral immunity is formed. Everything is great. Even the fact that such a vaccine costs 5–10 times more than a recombinant or whole virion vaccine, and requires special conditions of transportation, storage and use within a “continuous cold chain” (-70 C), does not reduce its importance - health is more expensive.
Such mRNA-based vaccines, as well as the recombinant vector vaccines discussed above, have been in development for almost 30 years, since the early 1990s. They are modified, improved and tested on cottontail hamsters, cynomolgus macaques, ferrets, guinea pigs, and show good results in the treatment of vesicular stomatitis in white mice.
Something else is alarming. Such vaccines have not yet been used on a large scale not only for the prevention of infectious diseases in humans, but also for the immunization of farm animals (not counting individual experiments on the immunization of dogs against rabies and pigs to obtain antibodies against the influenza virus). But both American companies quickly created and brought to registration systems for the production of mRNA vaccines against the S-protein of SARS-CoV-2 within 9 months. According to American sources, both vaccines showed high effectiveness in all groups of subjects in a number of countries, regardless of the age, gender or race of the people vaccinated with them. However, for people over 65 years of age, the effectiveness of one of these vaccines was 94%. The elderly tolerated the vaccine more easily and complained less often about side effects. This refers, of course, to short-term side effects, but not long-term side effects, the existence or absence of which is not known for mRNA-based vaccines for the reasons described above. And this is also somewhat worrying.
Return
Vector vaccines
What is this? Vaccines are based on completely different viruses (for example, adenoviruses), into which a small gene is embedded - a section of the SARS-CoV-2 genome. As a result, SARS-CoV-2 antigen proteins appear in the shells of harmless viruses (they are called “vectors,” that is, transport for delivery into cells).
What is the mechanism of action? Once in the body along with the vaccine, genetically modified auxiliary viruses provoke an immune response to SARS-CoV-2 proteins - that is, they work approximately like “live” viral vaccines.
Theoretically, it is possible to try to create two types of vector vaccines - based on viral particles that are capable of and those that are not capable of reproducing in the body. Most likely, vaccines based on viral particles that can reproduce inside the cells of the host body will protect against coronavirus longer. However, only vaccines with viruses that are not capable of reproducing have reached the stage of clinical trials on humans.
What's good about this vaccine? According to the developers' plan, vector vaccines should work as well as live ones, but at the same time they will not be able to mutate.
What's the problem with the vaccine? Vector vaccines based on attenuated genetically modified adenoviruses have not been sufficiently studied. Attempts have been made to develop vector vaccines to combat cancer, HIV, influenza and Ebola viruses, but none have yet been approved for use in humans.
Who is working on the vaccine and at what stage is it? According to WHO, as of April 30, 2021, two strong players are involved in vector viral vaccines.
The Chinese company CanSino Bio, together with the Beijing Institute of Biotechnology, is developing the Ad5-nCoV vaccine, based on a modified type 5 adenovirus. The vaccine is in the second phase of clinical trials - that is, testing of the vaccine on real patients has already begun. At the moment, CanSino Bio is the leader in the “vaccine race” - but this does not mean anything yet, because the global medical community has not yet seen the results of the first phase of trials. It is possible that there are a number of unreported problems with the vaccine.
The second strong player is the English University of Oxford, which is developing a vector vaccine based on a modified chimpanzee adenovirus ChAdOx1. The vaccine is in phases 1-2 of clinical trials - that is, it is also already being tested on real patients. Nothing much is known about ChAdOx1 yet. But another Oxford product based on the same principle—a vaccine against MERS-CoV, a “cousin” of the SARS-CoV-2 virus—appears to work and has had no safety problems.
Chapter 3
Production and description of the vaccine
The process of isolation and genetic characterization of the AYDAR-1 vaccine strain was previously presented [21]. The virus was filtered at the third passage and further purified by dilution. Primary, master and working seed batches of the strain (namely passage numbers 7, 8 and 9) were generated and characterized according to national vaccine production guidelines.
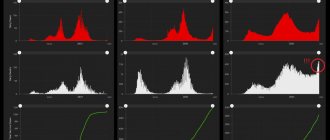
Figure 1 | The production process of the CoviVac vaccine and its authenticity
A - Basic sequence of the vaccine production process; B - Negative contrast transmission electron microscopy (TEM) of inactivated vaccine concentrate after chromatographic purification; selected particle (bottom right); C - Electrophoresis (SDS-PAGE) of the vaccine preparation (purified inactivated viral preparation after chromatography), stained with Coomassie blue; D — Western blotting of the viral preparation before inactivation and the vaccine preparation (purified inactivated viral preparation after chromatography) stained with human convalescent serum after COVID-19; E - Western blotting of a virus preparation before inactivation and preparation of the vaccine (purified preparation of inactivated virus after chromatography), stained with rabbit anti-S protein serum; F - culture of Vero cells infected with SARS-CoV-2 and stained with mouse serum immunized with the CoviVac vaccine (green staining in the microphotograph) and Hoechst 33342 (blue staining in the microphotograph); G , Vero cells infected with SARS-CoV-2 and stained with human convalescent serum from COVID-19 (green staining) and Hoechst 33342 (blue staining).
Transmission electron microscopy (TEM) (Fig. 1B) with negative contrast contrast concentrates revealed pleomorphic spherical viral particles with a diameter of about 120 nm, covered with spike-like structures 16–20 nm in length.
TEM (Fig. 1B) confirmed the homogeneity and purity of the vaccine preparation and identified virions with spike proteins that were consistent in shape and size with those identified in other studies [26, 27].
SDS-PAGE electrophoresis and Western blotting (WB) of pre-inactivation and post-chromatography vaccine concentrates stained with COVID-19 convalescent sera (Figure 1 C and D) identified two major proteins in the concentrates: N and S, which must also be contained in the virion preparation. Using anti-S protein serum staining (Fig. 1E), two forms of S protein were detected in viral preparations before and after inactivation: S1 and full-length S protein. This indicates that the vaccine preparation contains a target antigen for inducing NAb synthesis.
The specificity of antibody reactivity is confirmed by the absence of luminescence (fluorescence) in uninfected Vero culture cells.
Nucleic acid vaccines
DNA vaccines
What is this? A vaccine that contains a circular DNA molecule (plasmid) that contains the “instructions” for creating a viral protein.
What is the mechanism of action? Once in the cells of the grafted person, the circular DNA will become part of their genome. As a result, the cells of the host body will receive new instructions, according to which they will begin to “stamp” viral proteins-antigens - and an immune response will be formed to them.
To ensure that a piece of DNA with information about viral proteins penetrates cells, it can be inserted into the genome of a harmless carrier virus. This virus works like an “intracellular syringe” - it throws its modified genome into the cell, which is then integrated into the nucleus (unlike vector vaccines, here only the shell is used from a harmless virus).
What's good about this vaccine? The advantages are the same as those of vector vaccines: immunity is as durable as that of “live” viral vaccines, but without their inherent disadvantages. Since SARS-CoV-2 is not taken as the “carrier virus” for the plasmid, there is no danger that the weakened virus will mutate and cause the disease again.
What's the problem with the vaccine? DNA vaccines are poorly studied. So far, only one vaccine of this type is used - the Zika virus vaccine for horses. No DNA vaccine has yet been approved for use in humans.
Who is working on the vaccine and at what stage is it? According to WHO, as of April 30, 2021, Inovio Pharmaceuticals (Pennsylvania, USA) is creating a DNA vaccine INO-4800 - only based on DNA plasmids, without modified carrier viruses. INO-4800 is a so-called electroporation DNA vaccine. To “drive” the plasmid into muscle or skin cells, they will need to be exposed to an electric field, which will temporarily make the cell membranes more permeable. To make such a vaccination, a simple syringe will not be enough - you will need a special electroporator device. This vaccine is in phase 1 clinical trials, with trial results expected in June.
RNA vaccines
What is this? A vaccine that contains a viral molecule similar in structure to DNA - messenger RNA (mRNA). This molecule is a “template” from which the viral protein is directly read. mRNA is not integrated into the cellular genome.
What is the mechanism of action? The mRNA enclosed in a lipid nanoparticle enters the body along with the vaccine. Then the lipid particle will merge with the membrane of the target cell, and its contents will enter the cell and turn into a “template” for the synthesis of viral antigen proteins. As a result, the body’s own cells will begin to synthesize viral proteins, although the viral DNA will not be integrated into the cellular genome.
What's good about this vaccine? In addition to the benefits they share with DNA vaccines, the lipid particles with the mRNA inside are virus-like, so they can trigger an immune response on their own. There is a chance that due to the “double action”, immunity from RNA vaccines will occur earlier and last longer. In addition, short mRNA is a very simple molecule, so it can be created relatively quickly and inexpensively using special synthesizers.
What's the problem with the vaccine? This is a completely new vaccine - so we have no idea how it will behave in the human body. In principle, older vaccines of this type do not exist.
Who is working on the vaccine and at what stage is it? According to WHO, as of April 30, 2021, two companies were the furthest along in creating RNA vaccines. The American company BioNTech has signed a contract with the pharmaceutical giant Pfizer. However, other than the fact that the company received permission to begin phase 1-2 clinical trials in Germany, little is known about the vaccine. However, representatives reported that their vaccine could be ready by the fall of 2021.
More information about the vaccine from the American company Moderna, which is collaborating with the National Vaccine Research Center (NIAID). The vaccine is called mRNA-1273. The first phase of trials recently ended, which involved three vaccine options with mRNA concentrations of 25, 100 and 250 micrograms. The company has now submitted an application for a second phase of testing, which will involve the vaccine in dosages of 50 and 250 micrograms - perhaps these are the dosages that have proven to be the most effective.
In addition, in mid-March the Russian biotechnology company BIOCAD announced the start of development of an RNA vaccine. Three vaccine options with different mRNA dosages will be developed. The first animal trials were planned to begin at the end of April.
Chapter 4
Protein vaccines
What is this? A vaccine based on antigen proteins, that is, “pieces” of the virus.
What is the mechanism of action? When a mixture of viral antigen proteins enters the body along with the vaccine, it provokes an immune response.
What's good about this vaccine? This vaccine is safe for the body, so it can be quickly tested and put into use.
What's the problem with the vaccine? It is very difficult to obtain enough viral proteins to make a vaccine. In addition, immunity to such vaccines is likely to be unstable - much like in the case of inactivated vaccines.
Who is working on the vaccine and at what stage is it? According to WHO, as of April 30, 2021, no protein vaccine has yet crossed the threshold of preclinical trials. And if it does, it is unlikely that such vaccines will become widespread. Although, in theory, the possibility of producing viral proteins in large quantities exists - for example, Sanofi has a technology that allows them to “stamp” the proteins of influenza viruses in the cells of caterpillars. But making vaccines this way is very expensive and difficult.
Chapter 5
Immunity and its resistance
The short-term immunogenicity of the CoviVac vaccine was assessed in three animal models (two genetic strains of mice, Syrian hamsters and common marmosets) immunized with different doses. The vaccine induced NAb synthesis in all species studied. Moreover, antibodies to the two main structural proteins of the virus (S and N) were detected in mice. During the first 2–4 weeks, no significant differences were observed between the titers of NAbs, the synthesis of which was caused by different doses of antigen. Differences appeared starting from the fifth week after the first immunization.
As noted above, NAb synthesis is one of the main markers of protection against SARS-CoV-2 [8]. Therefore, the duration of the antibody response (NAb) correlates with the duration of protection. After natural infection, especially in cases of mild infection, the response in the form of NAbs is rather weak and short-lived [11].
There is very little information about the durability of vaccine-induced immunity. Although published preclinical studies have demonstrated the induction of SARS-CoV-2 IgG IgG and NAb titers following the administration of various vaccines, few studies provide data on the duration of the immune response. For example, for the drug PiCoVacc (an inactivated vaccine), the results of preclinical trials have been published, according to which the antibody titer after vaccination in mice and rats persists for six weeks, and in rhesus macaques - up to three weeks [25]. In the work published by Wang et al., the immunogenicity analysis in animals was limited to four weeks [27].
For the BBV152 vaccine candidate, immunogenicity measurements in the three-dose regimen were performed up to day 25 [29]. The authors assessed long-term immunogenicity in mice and marmosets over one year. During this period, no significant decrease in NAb titers was detected. Lower doses of administered antigen resulted in the formation of a lower NAb titer over a long observation period. While it is clear that definitive knowledge about the duration of immunity provided by COVID-19 vaccines will come from long-term clinical studies, animal models may serve as useful surrogate indicators early in the vaccine development process. A recent study of Moderna's mRNA vaccine clinical trial reported elevated specific antibody titers for at least three months [30]. According to the experimental data of the authors of the article, the CoviVac vaccine ensured the formation of stable long-term immunity in mice and marmosets after a two-component drug administration regimen.
Why do vaccines take so long to develop?
Creating vaccines is very difficult and expensive . The creation of vaccines requires not only highly qualified personnel and large financial investments in research; the problem is also in establishing production. To bring a vaccine to market, small development companies will have to reach an agreement with large pharmaceutical companies, which will be able to produce components for the drug in large quantities. At the same time, the production of a completely effective vaccine may turn out to be too difficult to become widespread - we have already seen this with the example of protein vaccines. Due to production difficulties, 95% of vaccines that have successfully completed clinical trials do not reach consumers.
Clinical trials of vaccines take a long time . A successful vaccine is one that will be used in tens of thousands, perhaps millions, of people. Therefore, all vaccine candidates must be thoroughly tested not only for effectiveness, but also for safety - because with such huge volumes, even rare side effects become very likely.
A good example is the risk of antibody-dependent enhancement (ADE), in which there is a theoretical risk that antibodies from a vaccine designed to fight one strain of coronavirus will facilitate infection by another strain of coronavirus. Scientists do not fully understand what properties of vaccines provoke ADE - so they just have to experiment and see whether this effect exists or not. Checking for ADE also takes time.
And although developers of vaccines (especially new ones - vector and vaccines based on RNA and DNA) are doing everything to speed up the development process, the stage of testing vaccines in humans - clinical trials - should not be skipped under any circumstances.
Clinical trials (even accelerated ones) take at least several months. It is required to recruit several dozen (or better yet hundreds) participants, randomly (this is called randomization) divide them into an experimental group that will receive the vaccine and a control group that will receive a placebo, and observe these people for at least 3-4 months so that they have time possible side effects may occur.
Chapter 6
Preventive effectiveness
Most recent studies have used the Syrian hamster as a convenient and reliably non-lethal animal model for the preventive efficacy of COVID-19 vaccines. In Syrian hamsters, SARS-CoV-2 infection causes significant pathological changes in the lungs and thus supports the development of a stable post-infectious humoral immune response in passive transfer experiments [35]. Moreover, the observed immunohistochemical changes and pattern of body weight loss in hamsters are similar to mild SARS-CoV-2 infection in humans [36]. A number of studies have demonstrated the suitability of the Syrian hamster as a model for studying the preventive efficacy of NAbs and vaccines against SARS-CoV-2 [37–46], although the symptoms of pneumonia in the animal develop quickly and are severe.
The Syrian hamster has been used as a model animal to evaluate the preventive efficacy of several inactivated vaccines [47–48], including those approved for clinical use [29]. The main evaluation parameters include the weight of the animal and the presence of the virus and/or viral RNA in swabs from the nose, lungs and other organs at different times after infection.
In the authors' study, animals from the control group lost weight until the fifth to seventh day after infection, while vaccinated animals gained weight starting from the third day after infection, which correlates with data on BBV152 [29]. However, weight loss in control animals in the authors' experiments was more pronounced - 15% versus 2-10% in the BBV152 study. The rate of clearance of viral RNA from the upper respiratory tract was also similar: from the seventh day after infection, most nasal swabs did not contain viral RNA. The level of viral RNA in the lungs of control animals was similar in both studies; According to the authors, the organs of all control animals contained viral RNA on the fourth, seventh and 14th days. The lung tissues of vaccinated animals were largely virus-free: only one out of five hamsters had detectable viral RNA in the lungs on days four and seven; however, by day 14, the lung tissue had cleared the virus. Viral RNA was detected in tissues other than the lung in animals of the control group only on the third day after infection. Similar results were obtained for the vaccine drug BBV152 [29]. Thus, the presented results demonstrate the preventive effectiveness of the CoviVac vaccine in the Syrian hamster model.
Thus, for the CoviVac vaccine, no signs of acute/chronic, reproductive, embryo- and fetotoxicity or teratogenic effects were found in the antenatal and postnatal periods of development, as well as signs of hypersensitivity in the animal species studied. The vaccine contributed to the formation of a stable and durable humoral immune response, both in the form of specific IgG to SARS-CoV-2 and NAbs in rodents and monkeys. There was no significant decrease in NAb titers over one year. CoviVac has demonstrated a preventive effect against SARS-CoV-2 infection in Syrian hamsters. These data encourage further study of the CoviVac vaccine in clinical trials.
When can we expect a vaccine to appear?
In the “pre-coronavirus era,” the development of one vaccine took on average more than 10 years. The only exception is the vaccine against the Ebola virus: Merck completed the development of this drug in a record five years. But in the midst of the COVID-19 pandemic, no country in the world has that much time, so government regulators and pharmaceutical companies are accelerating the development and testing of vaccine candidates - for example, the US government hopes to have a ready-made drug by early 2021.
If this really works out, it will be an unprecedented step forward for all of humanity. However, this is still not very likely. Considering all of the above, it makes no sense to wait for a vaccine against COVID-19 earlier than in 12-18 months.
By the way, a special website has recently appeared that aggregates information from the WHO, the American Centers for Disease Control and Prevention (CDC) and other sources: COVID-19 Vaccine & Therapeutics Tracker. The site is convenient for monitoring the development of vaccines in real time.