Review
Acute otitis media is most often a bacterial or viral infection that affects the middle ear, the air-filled space behind the eardrum that contains tiny vibrating bones. Children are more likely than adults to suffer from this disease.
Acute otitis media is often painful due to inflammation and fluid buildup in the middle ear.
Since ear infections often clear up on their own, treatment may begin with pain management and monitoring the problem. Otitis media in infants, and in severe cases in general, often requires antibacterial drugs. Long-term inflammation—persistent fluid in the middle ear and frequent infections—can cause hearing problems and other serious complications.
What is otitis media?
The middle ear is the cavity between the eardrum (the inner border of the outer ear) and the inner ear. Inflammation of the middle ear is called otitis media. This disease often develops in children due to the structural features of the ear, especially the Eustachian tube, and in the presence of adenoiditis. Otitis media is usually caused by bacteria or viruses.
IMPORTANT! Information from the article cannot be used for self-diagnosis and self-medication! Only a doctor can prescribe the necessary examinations, establish a diagnosis and draw up a treatment plan during a consultation!
Symptoms
Symptoms of inflammation usually develop quickly.
Signs and symptoms common in children include:
- pain in the ears, especially when lying down;
- poor sleep;
- crying more than usual;
- difficulty listening or responding to sounds;
- loss of balance;
- fever (38 C or higher);
- discharge of fluid from the ear;
- headache;
- loss of appetite.
Common symptoms in adults include:
- earache;
- release of fluid;
- hearing loss.
Symptoms of otitis media
In children:
- ear pain, especially when the child is lying down;
- “tugs” or “shoots” in the ear;
- the baby does not sleep, cries, is excited, restless;
- preschooler or schoolchild has no appetite, headache;
- decreased hearing (no reaction to sounds);
- imbalance;
- temperature is usually above 38.0;
- Fluid flows from the ear, which brings relief.
In adults:
- earache;
- hearing loss;
- Fluid flows from the ear, which brings relief.
Causes
Inflammation in the middle ear is caused by bacteria or viruses. Often caused by a cold, flu, or allergies, it causes fluid to accumulate and swell in the nasal passages, throat, and auditory tubes.
The role of the auditory tube
The auditory tubes are a pair of narrow tubes that extend from the middle ear to the nasopharynx, behind the nasal passages. The laryngeal end of the tubes opens and closes to regulate air pressure in the middle ear and its drainage function.
Swelling, inflammation, and mucus in the eustachian tubes from an upper respiratory infection or allergies can block them, causing fluid to accumulate in the middle ear.
Ear infections are more common in children, in part because their eustachian tubes are narrower and more horizontal—factors that make it difficult for fluid to drain out of them, causing them to become clogged.
Role of adenoids
Adenoids are two small pads of tissue high at the back of the nose that play a role in the activity of the immune system. This feature makes them especially vulnerable to infection, inflammation and swelling.
Because the adenoids are located near the opening of the eustachian tubes, inflammation or enlargement of the adenoids can block the eustachian tubes, thereby facilitating middle ear infection. Inflammation of the adenoids will play a role in the development of otitis media in children because children have relatively large adenoids.
Other conditions that may be associated with an ear infection or the result of similar middle ear problems include the following:
- Otitis with effusion is inflammation and fluid formation (effusion) in the middle ear without bacterial or viral infection. This can happen because fluid accumulation persists after the ear infection has cleared. It may also occur due to some dysfunction or non-infectious blockage of the eustachian tubes.
- Chronic otitis media with effusion occurs when fluid remains in the middle ear and continues to return without bacterial or viral infection. This makes children susceptible to new ear infections and can affect their hearing.
- Chronic suppurative otitis is a persistent ear infection that often leads to rupture or perforation of the eardrum.
Causes of otitis media
As already mentioned, otitis media is usually of a viral or bacterial nature. When, as a result of acute respiratory viral infections or allergies, the nose is stuffy and the throat is inflamed, the swelling can block the Eustachian tubes connecting the middle ear to the nasopharynx. Normally, the Eustachian tubes serve to “ventilate”, regulate pressure and secretion of the middle ear. In children they are narrower than in adults and have a smaller slope, so otitis media occurs more often.
Near the exits of the Eustachian tubes into the nasopharynx there are also adenoids - nasopharyngeal tonsils, which are often enlarged in children. Their inflammation can also provoke otitis media.
Risk factors
- Age. Children ages 6 months to 2 years are more susceptible to ear infections because of the size and shape of their eustachian tubes and because their immune systems are underdeveloped.
- Children's group. Children in group settings are more likely to get colds and ear infections than children who stay at home because they are exposed to more infections, such as colds.
- Baby food. Babies who drink from a bottle, especially while lying down, are more likely to develop ear infections than babies who are breastfed.
- Seasonal factors. Ear infections are most common during the fall and winter, when colds and flu are common. People with seasonal allergies are at greater risk of ear infections during seasonal allergies.
- Contaminated air. Exposure to tobacco smoke or high levels of air pollution can increase the risk of ear infection.
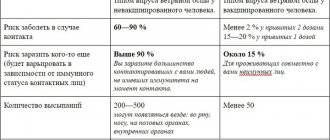
Side effects and complications after vaccines against otitis media, meningitis and pneumonia
Negative reactions after vaccination are possible. In children, after an injection, a lump is highly likely to appear in the appropriate place, which does not dissolve for several days.
This side effect is not dangerous, but it can cause great discomfort. In particular, a small child may cry often due to the painful sensations he experiences.
In rare cases, a person’s temperature rises after vaccination (usually by no more than 1 degree). Other effects: drowsiness and fatigue, or, on the contrary, increased psychomotor agitation, lack of appetite, irritability and chills.
The likelihood of developing these reactions is relatively low. Thus, lumps appear in only 5% of babies, and other effects occur in approximately 1% of people. There is no need to worry too much about the appearance of negative side effects. As a rule, they do not cause harm to health and go away on their own within 1-2 days.
If side effects cause severe discomfort, or they last a long time, then you need to contact the doctor who administered the vaccine. This will avoid complications, which can be very diverse.
Complications
Frequent infections and constant build-up of fluid can lead to serious complications:
- Hearing impairment. An ear infection is often accompanied by mild hearing loss. Persistent infection or fluid in the middle ear can lead to more significant hearing loss. If there is some permanent damage to the eardrum or other structures of the middle ear, permanent hearing loss may occur.
- Delayed speech development. When hearing is temporarily or permanently impaired in infants and young children, they may experience delays in speech, social and mental development.
- Spread of infection. Infections that do not respond well to treatment may spread to nearby tissue. Infection of the mastoid process, the bony protuberance behind the ear, is called mastoiditis. This infection can cause bone damage and pus-filled cavities. Rarely, serious middle ear infections spread to other tissues in the skull, including the brain or meninges surrounding the brain (meningitis).
- Rupture of the eardrum. Most tears heal within 72 hours. In some cases, surgery is necessary.
Prevention
The following tips may reduce your risk of developing otitis media:
- Prevent colds and other illnesses. Teach your children to wash their hands frequently and thoroughly, and not to share food or drinks. Teach your children to cough or sneeze into their hand. If possible, limit the time your child spends in a group setting. Try to keep your child at home when he is sick.
- Avoid secondhand smoke. Try to stay in non-smoking areas.
- Breastfeeding your baby. If possible, breastfeed your baby for at least six months. Breast milk contains antibodies that may provide protection against ear infections.
- If you bottle feed, keep your baby upright. Avoid propping bottles in your baby's mouth while he is lying down. Do not put the bottle in the crib with your baby.
- Talk to your doctor about getting vaccinated. Ask your doctor about which vaccines are appropriate for your child. Seasonal flu shots, pneumococcal and other bacterial vaccines can help prevent ear infections.
How to prevent otitis?
- Protect your child from ARVI. Teach children to wash their hands, not to drink from other people's dishes, and not to eat with other children's spoons.
- Choose breastfeeding. If you bottle feed, try to keep your baby from lying down while feeding. Don't give your baby a bottle in bed.
- Do not smoke in the room where the child is (do not take him to places where they smoke).
- Get your child vaccinated against pneumococcus and hemophilus influenza on time, and vaccinate your child against the flu. These types of bacteria and viruses cause, among other things, severe otitis media.
Diagnostics
Your doctor may diagnose an ear infection or other condition based on the symptoms you describe. To clarify the diagnosis and identify the cause of the disease, the doctor will use a special light-up instrument (otoscope) to look at the ears, throat and nasal passages.
Otoscopy
An otoscope is a specialized instrument that allows the doctor to examine the ear cavity and judge the presence of fluid behind the eardrum. Using an otoscope, the doctor can gently blow air against the eardrum. Typically, this air causes the eardrum to move. If the middle ear is filled with fluid, the doctor will hardly notice any movement of the eardrum.
Additional tests
Your doctor may perform other diagnostic tests if there is any doubt about the diagnosis.
- Tympanometry. This test measures the movement of the eardrum. The device that closes the ear canal regulates the air pressure in the canal, thereby causing the eardrum to move. The device quantifies how well the eardrum moves and a measure of the pressure inside the middle ear.
- Acoustic reflexometry. This test shows how the mobility of the eardrum changes in response to sound stimulation.
- Paracentesis. Sometimes the doctor may use a thin needle to pierce the eardrum to drain fluid from the middle ear, a procedure called paracentesis. If the infection does not respond well to previous treatment, then taking a smear of this fluid to determine the type of bacteria helps to choose the right antibiotic.
- Other tests. If your child has had persistent ear infections or persistent fluid build-up in the middle ear, your doctor may refer you to an audiologist, speech therapist, or therapist for testing of hearing, speech skills, language comprehension, or developmental abilities.
special instructions
The vaccine drug Menactra is recommended for use especially by people from risk groups who have an increased likelihood of developing meningococcal infection:
- people in direct contact with infected people;
- confirmed deficiency of properdin, complement components;
- tourists and those people who are going to visit areas unfavorable for meningococcal infection, located mainly in Africa;
- congenital or acquired absence of the spleen;
- accommodation in hostels, apartment-type hotels;
- people who are planning to serve in the army or are already recruits.
It is prohibited to combine the vaccine drug Menactra with any other drugs in the same syringe. Also, you cannot use subcutaneous, intravenous or intradermal methods of administering the vaccine. The studies conducted did not involve the use of the drug in people who have bleeding disorders and thrombocytopenia.
The vaccine is not used as a prophylactic against meningitis, which can be caused by other microorganisms or meningococci serogroup B. There have been cases of Guillain-Barré syndrome, which can progress after administration of the vaccine. Therefore, people who have previously suffered from this condition may be at risk of recurrence in the future. The decision to use the vaccine drug Menactra should be made by a doctor after assessing the possible risks of developing Siillain-Barré syndrome.
Patients who suffer from immune disorders and are being treated with immunosuppressive therapy may have a reduced immune response after using the vaccine.
Menactra has not been studied to affect driving.
What does the diagnosis mean?
Acute otitis media. The doctor makes this diagnosis if he observes signs of fluid in the middle ear, if there are signs or symptoms of infection, and if the onset of symptoms was relatively unexpected.
Otitis with effusion. If the diagnosis is otitis media with effusion, the doctor has detected fluid in the middle ear, but there are currently no signs or symptoms of infection.
Chronic purulent otitis media. If the doctor makes this diagnosis, it means that he has discovered that a persistent ear infection is leading to a rupture or perforation of the eardrum.
Treatment
Some ear infections resolve without antibiotic treatment. What's best for your child depends on many factors, including the child's age and the severity of symptoms.
Waiting tactics
Ear infections usually improve within the first two days, and most infections clear up on their own within one to two weeks without any treatment. The American Academy of Pediatrics and the American Academy of Family Physicians recommend waiting and seeing the outcome in the following cases:
- Children 6 to 23 months of age with mild internal pain in one ear for less than 48 hours and a temperature of less than 39°C.
- Children aged 24 months and older with mild internal ear pain on one or both sides for less than 48 hours and a temperature less than 39°C.
Some evidence suggests that antibiotic treatment may be effective for children with ear infections. Talk to your doctor about the benefits of antibiotics, their side effects, and the emergence of bacteria that are resistant to antibiotics when you overuse them.
Pain management
To reduce pain from an ear infection, your doctor may recommend using paracetamol (Calpol, Panadol, and others) or ibuprofen (Nurofen, Ibuclin, and others) to relieve the pain. Use medications as directed on the label. Use caution if giving aspirin to children or teenagers. Children and teenagers recovering from chickenpox or flu-like symptoms should never take aspirin because aspirin is associated with Reye's syndrome.
Antibiotic therapy
Your doctor may recommend treating otitis media with antibiotics in the following situations:
- Children 6 months of age and older with moderate/severe ear pain for more than 48 hours or a temperature of 39°C or higher.
- Children 6 to 23 months of age with mild internal ear pain lasting less than 48 hours and a temperature less than 39°C.
- Children aged 24 months and older with mild internal ear pain lasting less than 48 hours and a temperature less than 39°C.
In children under 6 months of age with confirmed acute otitis media, treatment should be started with antibiotics without an initial wait and observation period. Even after symptoms have improved, be sure to complete the course of antibiotics as recommended. Failure to follow this recommendation may result in recurrent infections and bacterial resistance to antibiotic therapy. Talk to your doctor about what to do if you accidentally miss an antibiotic dose.
Bypass surgery
If your child has recurrent otitis media or otitis media with effusion, the doctor may recommend a procedure to remove fluid from the middle ear. Recurrent otitis media can be said to occur if there have been three episodes of infection in six months or four episodes in a year, or at least one episode in the last six months. Recurrent otitis with effusion is a constant build-up of fluid in the ear after recovery or in the absence of any infection.
During an outpatient surgical procedure called a shunt, the surgeon creates a tiny hole in the eardrum that drains fluid from the middle ear. A tiny tube (shunt) is placed in the hole to help ventilate the middle ear and continue to drain fluid for the required amount of time. The shunt is installed for 3-6 months and removed surgically. The eardrum usually closes again after the shunt is removed.
Treatment of chronic suppurative otitis media
Chronic suppurative otitis media leads to perforation of the eardrum and is difficult to treat. It is often treated with antibiotics given as drops.
Ear infections. How to avoid otitis media
04.Feb.2021
An infection in the middle ear (the space behind the eardrum where tiny bones pick up vibrations and transmit them to the inner ear) very often accompanies colds, flu, or other types of respiratory infections. This is because the middle ear is connected to the upper respiratory tract by a tiny canal known as the eustachian tube. Germs and viruses that multiply in the nasal cavity or sinuses can travel through the Eustachian tube and into the middle ear. Ear infections are the most common reason for visits to the ENT doctor.
Today, nearly half of all antibiotic prescriptions written to children are for ear infections. Left untreated, ear infections can lead to more serious complications, including mastoiditis (a rare inflammation of the bone adjacent to the ear), hearing loss, perforated eardrum, meningitis, and facial paralysis.
What causes ear inflammation?
The middle ear is a small space behind the eardrum that should be well ventilated with air that usually passes up from the nose through the Eustachian tube, keeping the middle ear clean and dry. When there is not enough fresh air to ventilate the middle ear, such as when the Eustachian tube is clogged or blocked, the area becomes moist, stagnant and warm, an ideal breeding ground for germs.
In children and infants, the Eustachian tube is often too soft and has a harder time staying open. Sinus infections, viruses, and adenoid vegetations can affect the eustachian tube's ability to pass air into the middle ear.
In children, ear infections most often occur due to acute respiratory viral infections. These diseases can cause the Eustachian tube to become so swollen that air can no longer enter the middle ear. Allergies (to pollen, dust, animal dander, or food) can cause the same effect, as can smoke, fumes, and other environmental toxins. Bacteria can directly cause an ear infection, but usually these organisms follow a viral infection or allergic reaction, quickly infiltrating the warm, moist environment of the middle ear. The bacteria most commonly found in an infected middle ear are the same species that cause many cases of sinusitis, pneumonia, and other respiratory infections.
Ear infections occur in different ways. An isolated case is called acute otitis media. If the condition goes away but then returns three times within 6 months (or four times a year), it is called recurrent acute otitis media. This usually indicates that the function of the eustachian tube is impaired. A buildup of fluid in the middle ear without infection is called otitis media with effusion, a condition in which fluid remains in the ear because it is poorly ventilated but germs have not yet begun to grow.
In recent years, scientists have identified the characteristics of people most likely to suffer from recurrent middle ear infections:
— Persons with a family history of ear infections — Formula-fed children (breastfed children have fewer ear infections) — Children attending day care centers — People who are second-hand smokers — People with palate abnormalities (such as cleft palate) ) - People with poor immune systems or chronic respiratory diseases such as cystic fibrosis and asthma.
What are the symptoms of inflammation in the ear?
In children, the symptoms are as follows: • Poor sleep • Increased body temperature • Irritability, restlessness • Fluid discharge from the ear • Decreased appetite • Cries at night when lying down
Contact your doctor immediately if:
• Your child has a stiff (increased muscle tone) neck. • Your child is very lethargic, does not respond well to communication, or cries.
Tips for preventing ear infections.
Ear infections tend to occur more often in the fall and winter because upper respiratory infections such as colds and flu increase at the same time. Children 2 years of age and younger are more likely to get ear infections due to the small size and shape of the eustachian tube.
What else can cause otitis media?
Bottles and pacifiers: If babies drink from a bottle, lie down, or use a pacifier, they are more likely to get ear infections. Daycare centers: Children may be exposed to more germs in situations where there are a lot of them. Air quality: Cigarette smoke and other types of air pollution can increase your child's chance of getting an ear infection.
In order to reduce the likelihood of your child getting sick, you need to:
Breastfeeding (infants who breastfeed for 12 months or more tend to have fewer infections). If breastfeeding is not possible, bottle feed your baby while sitting upright. Fresh air - do not smoke in the presence of a child. If possible, try to avoid other forms of air pollution. Immunization – follow the mandatory vaccination schedule. Throw away pacifiers – If your baby uses a pacifier after 12 months, the likelihood of developing ear infections increases. Do everything you can to wean your baby off them. Wash your child's hands and yours often with soap. This can reduce the spread of germs and prevent your baby from contracting viral infections. Another tip, even though it can be very difficult: try to keep dirty objects away from your baby's mouth. If your doctor decides to prescribe antibiotics, follow all instructions. Take all doses, even if you or your child feel better. Check with your doctor if you feel unwell from the medicine. If you do not complete the entire course of treatment and do not follow all the doctor's recommendations, your infection may return and become resistant to new treatments. If the infection is causing serious complications, fluid remains in the ear for a long time, or your child has an ear infection that keeps coming back, the doctor may do a procedure called a myringotomy. A small hole is created in the eardrum, into which a small tube is inserted. It may leak fluid (such as effusion, blood, or pus). The tube, which provides ventilation and drainage, usually falls out on its own after about 6 to 18 months.
In order not to experience pain and not to listen to the signals that the body gives, it is better to take preventive measures in advance. It's not complicated. You should wear a hat in the cold season, do not avoid gloves and scarves, and keep your feet warm. In addition, it is worth increasing the body's defenses, drying your hair after visiting the pool, and taking vitamins.
I. Arteev, doctor - otorhinolaryngologist