Why should children be vaccinated with BCG?
How do you feel about the trend to refuse vaccinations?
Frankly, I'm pretty tired of these conversations. Whether or not to vaccinate a child is the parents’ choice, but they must bear responsibility for the decision made. We have decided to shift all responsibility onto doctors. In the late 1990s, I studied in the USA, and I was amazed at how the relationship between patient and doctor was built there. The doctor’s task is to tell the patient or his parents about the possible consequences of a particular action. A person receives information, then goes to the library, which is often located in the same clinic, and makes a decision on his own. This approach is close to me. If parents don't want to get vaccinated, that's their business. But please, first study information from competent sources, and not just what you want to hear. Weigh all the pros and cons, all the risks. Unfortunately, parents often refuse vaccinations not after studying medical literature and consulting with doctors, but after reading the opinions of ordinary people on the Internet.
Let me give you an example: the population of St. Petersburg, the Leningrad Region and Finland is approximately the same. Moreover, during the period 2009 - 2010, 6 children with bone complications of BCG vaccination were identified in two of our regions, and not a single one in Finland, where there is no mandatory BCG vaccination. What conclusion would you draw from this information?
Of course, “why do we need these vaccinations?”
Right. But here’s a nuance: during the same period in Finland, two children fell ill with tuberculous meningitis (damage to the meninges), and one child died, while in St. Petersburg - not a single one. Your opinion has changed, right? Of course, even if you are vaccinated you can get tuberculosis. But BCG vaccination does not aim to 100% prevent tuberculosis - it prevents the development of its severe forms. Without it, the likelihood of contracting such tuberculosis increases significantly. It is safe to refuse vaccinations in countries where the incidence of tuberculosis according to the WHO classification is low. Unfortunately, Russia does not fall into this group. The migration factor plays a major role: the more people come from regions where the incidence of tuberculosis is high, the higher the risk.
In Europe, the migration situation has recently worsened to the limit. But at the same time, in many European countries, BCG vaccination is not included in the vaccination calendars.
Take the test
Is your child ready for school?
Why does my head hurt?
It is too early to talk about the epidemic consequences of the wave of migration that we have seen in Europe in recent months. I think we will learn a lot of new things in the near future. Most migrants coming to European countries live in a closed group, which becomes a hotbed of infection. In Finland, for example, coming from a country with a high or moderate incidence of tuberculosis or having fairly close contact with such a person is an indication for BCG vaccination. I think that some countries that are currently experiencing a high migration burden will soon be forced to change their vaccination calendars. Otherwise, the consequences may be unpredictable.
Do I understand correctly that if the family is prosperous, the child is taken care of and there is no constant contact with the sick person, the likelihood that he will get sick is not high?
The influence of social factors on the risk of developing tuberculosis has long been proven. But even a child from the most prosperous family cannot live in constant isolation - he ends up in a children's group, on public transport, and may encounter a patient who himself does not know about his illness. A vaccinated child has a significantly lower risk of getting sick from such contact than an unvaccinated child. Parents should know what the disease can lead to - this is the most compelling argument that should be taken into account. This applies to any vaccination, and anti-tuberculosis vaccination in particular.
How do complications occur in children after BCG vaccination?
First you need to understand the mechanism of their occurrence. The BCG vaccine is a special strain of weakened (scientifically attenuated) live mycobacteria that spread throughout the body and irritate the system responsible for the formation of immunity. In response, the body develops resistance to these or similar bacteria. . For a number of reasons, for example, trauma, this process sometimes becomes pathological, and a focus of destruction appears in the bone. Most often, such lesions appear in long tubular bones, but can be in any part of the skeleton. This can happen at any time before age 3. Moreover, the process can proceed hidden for quite a long time.
Are there statistics: how many children get complications after BCG vaccination?
Vaccinations
I am a phthisiatrician with 30 years of practical experience.The first time I thought about the negative effect of the BCG vaccine on the body of newborns was in the 60s and 70s. Then, cases of left-sided axillary lymphadenitis caused by the BCG vaccine began to appear more often than before 1962. As you know, intradermal BCG vaccination was introduced in 1962. After this, young children appeared, patients with chronic granulomatous disease (CGD), who necessarily had left-sided axillary lymphadenitis-BCG. In the practice of pediatric surgeons, especially since 1965, frequent cases of destructive staphylococcal pneumonia began to appear, and in the practice of pediatricians - dysbiosis. Professor G. A. Samsygina confirms today, in 1996, that by the end of the 70s the frequency of bacteriosis increased 15 times, but, unfortunately, she does not connect this with BCG vaccination.
Despite the efforts of pediatricians, using a rich arsenal of new strong drugs cannot reduce the number of pustular and purulent-septic diseases in children in the first year of life. It was not possible to share such thoughts with any of the TB specialists - they were all staunch supporters of... plans brought down from the Ministry of Health. A kind of “taboo” was imposed on any objection to this. Therefore, I decided to contact the head of the department of childhood infectious diseases, academician of the USSR Academy of Medical Sciences, Professor N.I. Nisevich. After listening to me, she recommended contacting the deputy. minister... and I went through the authorities. Having familiarized themselves with my opinions about the dangers of BCG for the body of newborns, they frankly admitted that they had not imagined the possibility of the existence of such a point of view, but... they could not help in any way.
When my tuberculosis department learned about my visit to the Ministry of Health, a party group was assembled and a party punishment was announced for me. Nevertheless, I continued to express my thoughts in “Office Letters” and even in articles in the journal “Pediatrics”.
The fact is that mycobacteria tuberculosis are constant “companions” of a person only after he reaches a certain age, but not during the neonatal period
.
For adults, over the centuries-old history of mankind, Mycobacterium tuberculosis (on the Eurasian continent) has become an environmental environmental factor. Naturally, under these conditions, humans have also developed genetically fixed certain mechanisms of protection against Mycobacterium tuberculosis (MBT) - the so-called natural resistance to MBT has formed, thanks to which the majority of those infected with MBT either do not get sick with tuberculosis at all
, or
are cured
of the primary forms on their own, but how rule with the formation of residual changes, etc.
Regardless of the degree and form of primary infection of the office, in any case, they are fixed in various organs
(!), mainly in the reticuloendothelial system. Consequently, a similar picture is observed with BCG vaccination.
...I especially remember 3-year-old Sasha G., who was admitted to the First Children's Tuberculosis Hospital in the late 70s with a diagnosis of “Left-sided axillary lymphadenitis caused by the BCG vaccine, chronic granulomatous disease (CGD).” Previously, he had been treated for a long time and unsuccessfully in the tuberculosis hospital for young children No. 9. He was a well-fed, fair-haired, blue-eyed boy from young, healthy parents. They never had tuberculosis patients in their family. His disease, along with purulent-caseous left-sided lymphadenitis, was characterized by recurrent purulent otitis, purulent lymphadenitis of the cervical lymph nodes, and pustular skin lesions; culture of pus gave growth of staphylococcus. An enlarged liver was detected. Antibacterial therapy had no noticeable effect.
Considering my bitter inability to help this child, I achieved his transfer to the Central Institute of Tuberculosis. But it was not possible to help there either, because he had a failure of the phagocytosis reaction
. Some time later he died...
I have accumulated a significant number of similar cases. And what is characteristic is that more often these are boys, seemingly healthy in appearance, from quite wealthy families, fair-haired and light-eyed...
L.A. Mitinskaya and other authors of parenteral administration of the BCG vaccine to newborns claim that BCG is not to blame for the development of CGD, that BCG is only a marker of this disease. In other words, with the help of BCG and its complications, we are artificially selecting newborns who will definitely get sick? In contrast, I have become convinced that BCG, by delaying the development of the completed phagocytosis reaction, creates the conditions for the development of CGD in children of a certain genotype (blond-haired and blue-eyed).
Today, 31 children are being treated in our department, 23 of them are young. Moscow children - 6, residents of the Moscow region. - 4, from various regions of Russia - 9, from CIS countries - 10, foreigners - 2.
Of the six Moscow children, two are being treated due to a complicated course of BCG infection (one child has BCG osteitis of the sternum, the second has axillary lymphadenitis). The most severe condition is the condition of a 4-month-old child vaccinated with BCG in the maternity hospital. His mother was diagnosed with cavernous tuberculosis in the second week after being discharged from the maternity hospital (how did she end up in the maternity hospital with such a diagnosis?!). Her boy has general acute miliary tuberculosis, tuberculosis of all groups of intrathoracic lymph nodes, and the prognosis is very unfavorable...
Over 30 years of work, starting in 1970, we began to receive children with bone lesions, which were previously considered as manifestations of BCG infection. But it is not always possible to prove this due to the therapy performed, treatment with antibiotics, and therefore it is extremely difficult to carry out successful typing of mycobacteria BCG... Most of these children were operated on in Children's Clinical Hospital No. 13, and in recent years - at the Institute of Phthisiopulmonology in St. Petersburg. In some cases, typing confirmed the connection of bone lesions with BCG vaccination.
What does it mean to intradermally administer a “weakened” version - BCG-M, which, meanwhile, contains 500 thousand mycobacteria, i.e. the same amount that is part of BCG? In any case, they all remain in the body of children, who usually have different susceptibility to tuberculosis, because “polyomorphism and species viability were provided by biomolecules that made each of us unique. The genes in charge of the kaleidoscope of these proteins determined the most functionally diverse physiological system - the immune system, and with it the independence of individual life" (Govallo V.I. Why are we not alike each other
. M.: Knowledge, 1984, p. 134).
Yes, and BCG is heterogeneous in its content of mycobacteria, which differ in “weakened” virulence.
Having entered the child’s body, MBT immediately spreads into the lymph and blood and, naturally, multiplies, although they are weakened in the composition of BCG. In a day there will be not 500 thousand, but a million, in two days - 2 million, etc. In other words, BCG bacteremia occurs in the body of newborns, which will increase in each child differently. In the end, after a certain time, the baby “excites” its own delayed-type hypersensitivity reaction - PCHT. BCG vaccination is carried out precisely for this purpose - in order to excite this hereditarily determined reaction. As a result, by the end of the first week the child is literally “flooded” with BCG mycobacteria, which are strict aerobes that require constant oxygen. According to A.D. Ado and A.N. Mayansky, MBT are able to inhibit the formation of phagocytosis of phagolysosomes, and then this mechanism, which eliminates contact with the cytotoxic components of phagocytes, ensures long-term persistence of the weakened tuberculosis bacillus in macrophages. These authors point out that “complete phagocytosis requires the presence of biological oxidants with potent cytotoxic potentials” and that “due to the phenomenon of respiratory or metabolic burst, the digestion of certain microbes occurs, in particular Staphylococcus aureus and fungi. In an anaerobic environment, although phagocytes retain the ability to absorb, they sharply reduce toxicity against many pathogenic and opportunistic microbes" (Ado A. D., Mayansky A. N. Current state of the doctrine of phagocytosis
// Immunology, 1981, No. 3, p. 20).
Based on what is quoted, it is probably necessary to recall what has been well known for a long time that in newborns, phagocytosis is not yet mature enough qualitatively. If the absorptive capacity of phagocytes in newborns is sufficiently developed, then the final phase of phagocytosis is still imperfect and is formed at a much later date (and individuality should also be taken into account here!). In children of the first 6 months. life, the content of lysozyme, lactoferron, myeloperoxidase, etc., involved in the final phase of phagocytosis, is very low. Therefore, children in the first months of life have a high tendency to diseases caused by Staphylococcus aureus, E. coli, and fungi (Mazurin A.V., Vorontsov I.M. Propaedeutics of childhood diseases
. M., 1985, p. 264).
Thus, BCG vaccination is carried out for children with an unestablished reaction of completed phagocytosis, with an imperfect system of antibody formation - immunoglobulins, who have not adapted to the environment.
My many years of experience working with children of all ages, and in the last decade mainly with young children, led me to the final conviction of the need to stop BCG vaccination of newborns. This vaccination must be postponed to an older age, for a 2-3 year period of life, exclusively in endemic areas (which our sanitary and epidemiological service must determine!).
In my deep conviction, based on many years of practical work with post-vaccination complications after BCG vaccination, abandoning the universal vaccination of newborns is one of the main keys to solving the problems of reducing childhood morbidity and mortality.
Isn’t it scary to refuse vaccination of newborns in the context of a worsening epidemiological situation regarding tuberculosis?
I answer: not only is it not scary, but it is also necessary!
Firstly,
BCG vaccination has never prevented and cannot prevent a child from becoming infected with MTB if he is in contact with a patient with tuberculosis.
Secondly,
Without appropriate diagnosis of the state of the immune system, with the help of BCG we spread tuberculosis and accumulate it over generations among people susceptible to MTB, who are not all in disadvantaged social conditions.
Third
, all young children, regardless of the fact of vaccination, if they are susceptible to tuberculosis and infected in the maternity hospital, will definitely develop tuberculosis in the absence of timely diagnosis and treatment. There are no examples of self-healing from tuberculosis at this age. Self-healing is possible, however, only in children over 3 years of age.
Fourth
, the rate of MTB infection by two years remains at the level of 0.005–0.01%, i.e. 10:100,000. All these children can be cured if diagnosis is carried out in a timely manner and treatment is carried out with the utmost care and long-term observation.
Fifthly
, without BCG in maternity hospitals, young children will grow up healthy! Hence, including the massive acquisition of immunodeficiency syndromes (AIDS), if not initially, then actively acquired as a cause-and-effect development after BCG, as well as the development of numerous other symptoms of general pathology.
MBT, I repeat, have long been a significant factor in natural selection and the encounter with them (infecting a person) is programmed. A protective response is also programmed, primarily from the lymphatic system. But if such an encounter occurs in the form of BCG vaccination during the neonatal period, then one can expect undesirable and very severe consequences from the lymphatic system - up to leukemoid and even leukemic reactions...
As a clinician and phthisiatrician, I am convinced that postponing the timing of BCG vaccination to an older age will not only be the best protection against tuberculosis, but will also become a method of preventing leukemia in children...
In articles in the journal “Pediatrics,” I have repeatedly proposed holding a round table with the participation of leading phthisiatricians, pediatricians, immunologists, geneticists, microbiologists who know the basics of the immunology of infectious diseases, etc. to discuss the issue “ Inappropriateness
and the depravity of BCG vaccination during the neonatal period.”
Unfortunately, this did not happen. However, the first result has been achieved: the “taboo” from discussing this issue has been removed. Moreover, according to V.F. Uchaikin, the current chief infectious disease specialist of the country, the draft vaccination calendar he submitted to the Russian Ministry of Health provides for this important age feature (round table on the topic “The controversial problem of vaccination of newborns”
, held on February 17, 1997 in Scientific Center of Obstetrics, Gynecology and Perinatology).
You, dear Galina Petrovna, also participated in the discussion of this problem in this center.
The essence of my proposals, which I have been making for 20 years
, is to monitor indicators of physical development and health in three groups of children:
- Healthy newborns not vaccinated with BCG;
- Healthy newborns vaccinated with BCG;
- Children vaccinated with BCG with manifestations of dysbacteriosis, among them there are two groups: a) treatment with conventional methods; b) treatment using conventional methods with the addition of isoniazid at a dose of 8 mg/kg per day.
Carrying out this work does not require significant material costs, with the exception of the desire and time of performers who are truly interested in the health of the children of Russia and the nation as a whole. The work can be completed within a year.
BCG vaccination during the neonatal period is dangerous for the health and life of children.
In conclusion, I consider it necessary to once again emphasize that I am a staunch opponent of vaccination (any, not just BCG) during the neonatal period
, because the vaccine interferes with the development of natural (sanogenetic) reactions of the child: phagocytosis, antibody formation, adaptation to the external environment.
In addition, I believe, like many other experts, that there cannot be a single vaccination schedule for all children
. Moreover, it is impossible to introduce 8-10 vaccines into a child’s body: this is a disastrous practice designed to destroy the nation.
Vaccination should be carried out strictly according to epidemiological indications with the obligatory observance of contraindications that cannot be reduced - they need to be expanded, since there are practically no children belonging to the first health group, and this trend applies not only to newborns, but also to all age groups of children.
In my opinion, the private ruling of Judge A. A. Borshchev (the court on claims of parents in connection with post-vaccination complications - osteitis, in which you and I participated on December 10, 1996 as experts) is surprisingly very competent:
The court considers it necessary to issue a private ruling to the Ministry of Health and Medical Industry of the Russian Federation on the unsatisfactory state of vaccination of newborns. A private determination is not subject to appeal.
APPLICATIONS
- An official letter that has been in my possession for 16 years, with negative reviews from Nisevich N.I. and Mitinskaya L.A. Now I am passing it into your hands and to the Forensic Medical Examination Committee of Moscow.
- Journal article. "Pediatrics", 1984, No. 7.
- Journal article. "Pediatrics", 1996, No. 6.
With respect and admiration for your educational activities, Phthisiatrician of the highest qualification category, Ph.D. V. P. Sukhanovsky
Letter from an oncoimmunologist Letter from an obstetrician-gynecologist
Symptoms and signs
After 4-8 weeks, a tubercle forms in the armpit, which gradually increases in size. Its size is 10 mm or more, the skin over it is not changed, and the child’s general well-being is not affected.
Typical signs of post-vaccination lymphadenitis are:
- At first the formation has a soft texture, then becomes dense to the touch;
- Palpation does not cause pain;
- There is no increase in general and local temperature.
If the parents have not consulted a doctor, the tubercle in the center softens. Caseous masses form, which then break out. At the site of the tubercle, a fistula is formed, from which purulent contents are released.
When treatment is prescribed, after 2-3 weeks the inflammation of the lymph node subsides, and subsequently calcification occurs (deposition of calcium salts in the focal area) and the formation of a capsule.
With delayed treatment of lymphadenitis, the general condition of the child changes: intoxication develops, the temperature rises, anemia appears, and the liver increases in size.
A dangerous and very rare complication of vaccination is generalized BCG infection. The pathology develops with severe immune deficiency in the newborn. Generalization may be indicated by:
- Reaction from many groups of lymph nodes;
- Involvement of the skin and osteoarticular system;
- Polymorphic reaction from internal organs.
At autopsy, miliary tubercles and caseous decay are detected, from the foci of which mycobacteria of the vaccine strain are isolated. The generalized form of BCG infection can be fatal.
Treatment
To avoid serious complications from an abscess after BCG, treatment should begin at the first signs of its formation.
Several methods are used:
- At the early stage of the formation of a cold abscess, a bandage impregnated with Dimedxide (hormonal ointment) together with Rifampicin is applied to the site of its localization.
- When a size fluctuation of less than 15 mm occurs, the contents of the cold abscess are removed using a syringe. Then a 5% solution of Saluzide or Streptomycin is injected. This operation is performed at intervals of 2 days until complete recovery.
- The ulcer formed after the abscess is treated with a special powder - Isoniazid and covered with a sterile napkin.
Indications for surgery
A surgical operation to remove the abscess and the resulting capsule is performed for a chronic disease.
An abscess whose size exceeds 20 mm is removed in the following ways:
- opened with a scalpel;
- the capsule is excised;
- drainage is carried out.
Then a sterile bandage soaked in an antiseptic solution is applied. It is changed daily.
In addition to the procedures described, a therapeutic course is carried out, which involves the use of anti-tuberculosis drugs.
All identified cases of negative manifestations of vaccination are recorded in the clinic. Children with complications are under constant monitoring in the tuberculosis department. Every 6 months they are examined by a TB specialist.
In addition, they are observed by a pediatrician for 12 months. Any vaccines are strictly prohibited at this time.
What it is?
A cold abscess after a vaccine is a local response of the child’s body to the introduction of weak strains of tuberculosis bacteria.
This manifestation is a fairly common complication after vaccination. The abscess is localized directly in the place where the vaccine was given.
The vaccine is injected into the upper left shoulder.
This is a formation that does not cause pain or changes in the skin at the initial stage of development.
In some cases, a cold abscess (scrofuloderma) occurs with simultaneous enlargement of the lymph nodes under the arms. In the absence of timely treatment, an ulcer or, less commonly, a fistula forms at the site of the abscess.
An abscess forms very slowly: 2–6 weeks after vaccination.
Causes
BCG vaccination requires compliance with precautions, which include:
- mandatory medical examination of the baby in order to identify contraindications to the administration of the vaccine;
- biological properties of the administered tuberculosis strain, quality of the drug;
- the presence of a severe pathology that weakens the child’s immune system.
Violation of these requirements is the main reason that leads to complications in the form of an abscess.
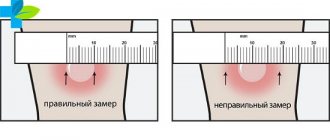
In addition, the most important is the human factor, namely, violation of the syringe insertion technique. Often, due to negligence, the vaccine is not administered intradermally, as required by the Instructions, but intramuscularly or subcutaneously.
This is what an abscess after BCG looks like in the photo: