Pharmacological properties of the drug Cytoflavin
A metabolic agent, the pharmacological effects of which are due to the complex effects of the components of the drug. Stimulates respiration and energy production in cells, improves the processes of oxygen utilization by tissues, restores the activity of antioxidant enzymes. The drug activates intracellular protein synthesis, promotes the utilization of glucose, fatty acids and resynthesis of GABA in neurons through the Roberts shunt. Cytoflavin improves coronary and cerebral blood flow, activates metabolic processes in the central nervous system, restores consciousness and intellectual-mnestic functions of the brain, eliminates reflex disorders and sensitivity disorders. It has a quick awakening effect during post-anesthesia depression of consciousness. When using Cytoflavin in the first 12 hours from the onset of stroke, a favorable course of ischemic and necrotic processes in the affected area (reduction of the lesion), restoration of neurological status and a decrease in the level of disability in the long-term period are noted. It has a positive effect on the parameters of neurological status: it reduces the severity of asthenic, cephalgic, vestibulo-cerebellar, cochleovestibular syndrome, and also eliminates disorders in the emotional-volitional sphere (reduces the level of anxiety, depression). Improves cognitive-mnestic functions and improves quality of life. With intravenous infusion at a rate of about 2 ml/min (in terms of undiluted Cytoflavin), succinic acid and riboxin (inosine) are utilized almost instantly and are not detected in the blood plasma. Riboxin (inosine) is metabolized in the liver to form glucuronic acid and its subsequent oxidation. A small amount is excreted by the kidneys. Nicotinamide is rapidly distributed in all tissues, penetrates the placenta and into breast milk, is metabolized in the liver to form nicotinamide-N-methylnicotinamide, and is excreted by the kidneys. The half-life from blood plasma is about 1.3 hours, the volume of distribution at steady state is about 60 l, and the total clearance is about 0.6 l/min. Riboflavin: distribution is uneven - the largest amount accumulates in the myocardium, liver, and kidneys. The half-life from blood plasma is about 2 hours, the volume of distribution at steady state is about 40 l, and the total clearance is about 0.3 l/min. Penetrates through the placenta and into breast milk. The degree of binding to blood proteins is 60%. Excreted by the kidneys, partly in the form of a metabolite; when administered in high doses - mainly unchanged.
Cytoflavin solution for injection. ampoules 10ml No. 10
Indications
In adults in complex therapy : 1. Acute cerebrovascular accident.
2. Consequences of cerebrovascular diseases (consequences of cerebral infarction, cerebral atherosclerosis). 3. Toxic and hypoxic encephalopathy in acute and chronic poisoning, endotoxicosis, post-anesthesia depression of consciousness, as well as for the prevention and treatment of hypoxic encephalopathy during cardiac surgery using artificial circulation. In children (including premature infants with a gestation period of 28-36 weeks) in complex therapy in the neonatal period: 1. For cerebral ischemia.
Directions for use and doses
In adults: CYTOFLAVIN® is used only intravenously in a dilution of 100-200 ml of 5-10% dextrose solution or 0.9% sodium chloride solution.
1. In case of acute cerebrovascular accident, the drug is administered as early as possible from the onset of the disease in a volume of 10 ml per injection with an interval of 8-12 hours for 10 days. In severe cases of the disease, the single dose is increased to 20 ml.
2. For the consequences of cerebrovascular diseases (consequences of cerebral infarction, cerebral atherosclerosis), the drug is administered in a volume of 10 ml per dose once a day for 10 days.
3. For toxic and hypoxic encephalopathy, the drug is administered in a volume of 10 ml per injection twice a day after 8-12 hours for 5 days. In a comatose state, a volume of 20 ml per injection diluted with 200 ml of dextrose solution. For post-anesthesia depression, once in the same doses. In the treatment of hypoxic encephalopathy during cardiac surgery using artificial circulation, 20 ml of the drug diluted with 200 ml of a 5% dextrose solution is administered 3 days before surgery, on the day of surgery, 3 days after surgery.
In children (including premature infants) in the neonatal period with cerebral ischemia, the daily dose of CYTOFLAVIN® is 2 ml/kg/day. The calculated daily dose of the drug is administered intravenously (slowly) after dilution in a 5% or 10% dextrose solution (in a ratio of at least 1:5). The time of the first administration is the first 12 hours after birth; The optimal time to start therapy is the first 2 hours of life. It is recommended to administer the prepared solution using an infusion pump at a rate of 1 to 4 ml/hour, ensuring a uniform flow of the drug into the bloodstream throughout the day, depending on the calculated daily volume of solutions for basic therapy, the patient’s hemodynamic state and acid-base parameters. The average course of treatment is 5 days.
special instructions
Administration of the drug to newborn (premature) children is carried out under the control of indicators of the acid-base state of capillary blood at least 2 times a day (both before and during therapy). Serum lactate and glucose levels should be monitored whenever possible. The rate of administration of a solution containing CYTOFLAVIN® should be reduced or temporarily stopped infusion in newborn (premature) children: - those on mechanical ventilation, when signs of mixed (respiratory-metabolic) alkalosis appear, which is threatened by the development of cerebrovascular accidents; - with preserved spontaneous breathing and respiratory support using the CPAP method or in those receiving an air-oxygen mixture through a mask when laboratory signs of metabolic alkalosis appear, which is threatened by the appearance or increase in frequency of apnea attacks. In patients with diabetes mellitus, treatment should be carried out under the control of blood glucose levels. Possible intense yellow coloration of urine. CYTOFLAVIN® does not affect the ability to drive vehicles.
Compound
1 ml of solution contains: active substances: succinic acid - 100 mg, nicotinamide - 10 mg, riboxin (inosine) - 20 mg, riboflavin mononucleotide (riboflavin) - 2 mg; excipients: N-methylglucamine (meglumine) 165 mg; sodium hydroxide 34 mg; water for injections
Contraindications
Hypersensitivity, in patients on mechanical ventilation, when the partial pressure of oxygen in arterial blood decreases to less than 60 mm Hg. Art., period of breastfeeding. With caution - nephrolithiasis, gout, hyperuricemia.
Use during pregnancy and breastfeeding
It is not recommended to take during pregnancy and lactation due to the lack of clinical data on the effectiveness and safety of the drug during this period
Side effects
With rapid drip administration, undesirable reactions may occur that do not require discontinuation of the drug: hyperemia of the skin of varying severity, a feeling of heat, bitterness and dry mouth, sore throat. Rare adverse reactions include: short-term pain and discomfort in the epigastric region and chest area, difficulty breathing, nausea, headache, dizziness, “tingling” in the nose, dysosmia, pallor of the skin of varying severity. Allergic reactions in the form of skin itching, transient hypoglycemia, hyperuricemia, and exacerbation of gout are also possible. In children (including premature babies) during the neonatal period, disturbances in the acid-base balance (alkalosis) may develop.
Overdose
To date, no cases of overdose with CYTOFLAVIN have been identified.
Storage conditions
In a place protected from light at a temperature of 0 - 25 ° C. Keep out of the reach of children.
Best before date
2 years.
pharmachologic effect
Pharmacodynamics Pharmacological effects are due to the complex effect of the components included in the drug CYTOFLAVIN®. CYTOFLAVIN® promotes activation of aerobic cell metabolism, which leads to an increase in the level of glucose utilization, promotes an increased level of beta-oxidation of fatty acids and the resynthesis of γ-aminobutyric acid in neurons. CYTOFLAVIN® increases the resistance of the membranes of nerve and glial cells to the effects of ischemia, which is expressed in a decrease in the concentration of neurospecific proteins that characterize the level of destruction of the main structural components of nervous tissue. CYTOFLAVIN® improves coronary and cerebral blood flow, activates metabolic processes in the central nervous system, restores impaired consciousness, promotes regression of neurological symptoms and improves cognitive functions of the brain. It has a quick awakening effect during post-anesthesia depression of consciousness. When using the drug CYTOFLAVIN® in the first 12 hours from the onset of stroke, a favorable course of ischemic and necrotic processes in the affected area (reduction of the lesion), restoration of neurological status and a decrease in the level of disability in the long-term period are observed.
Pharmacokinetics When administered intravenously at a rate of about 2 ml/min (in terms of undiluted CYTOFLAVIN®), succinic acid and inosine are utilized almost instantly and are not detected in the blood plasma. Succinic acid - the peak concentration is determined within the first minute after administration, with a further rapid decrease without cumulation and a return of its level to background values due to metabolization to water and carbon dioxide. Inosine is metabolized in the liver to form inosine monophosphate, followed by its oxidation to uric acid. A small amount is excreted by the kidneys. Nicotinamide is rapidly distributed in all tissues, penetrates the placenta and into breast milk, is metabolized in the liver to form N-methylnicotinamide, and is excreted by the kidneys. The plasma half-life is about 1.3 hours, the equilibrium volume of distribution is about 60 liters, and the total clearance is about 0.6 l/min. Riboflavin is distributed unevenly: the largest amount is in the myocardium, liver, and kidneys. The plasma half-life is about 2 hours, the equilibrium volume of distribution is about 40 liters, and the total clearance is about 0.3 l/min. Penetrates through the placenta and into breast milk. Communication with plasma proteins - 60%. Excreted by the kidneys, partly in the form of a metabolite; in high doses - mainly unchanged.
Drug interactions
Succinic acid, inosine, nicotinamide are compatible with other drugs. Riboflavin: Reduces the activity of doxycycline, tetracycline, oxytetracycline, erythromycin and lincomycin. Not compatible with streptomycin. Chlorpromazine, imipramine, amitriptyline, by blocking flavinokinase, disrupt the incorporation of riboflavin into flavin adenine mononucleotide and flavin adenine dinucleotide and increase its excretion in the urine. Thyroid hormones accelerate the metabolism of riboflavin. Reduces and prevents the side effects of chloramphenicol (disturbance of hematopoiesis, optic neuritis). Compatible with drugs that stimulate hematopoiesis, antihypoxants, and anabolic steroids.
Use of the drug Cytoflavin
Only IV drip diluted in 100–200 ml of 5–10% glucose solution or 0.9% sodium chloride solution. In case of acute cerebrovascular accident, the drug is administered as early as possible from the onset of the disease in a volume of 10 ml per injection with an interval of 8–12 hours for 10 days. In severe cases of the disease, the single dose is increased to 20 ml. For discirculatory encephalopathy and the consequences of cerebrovascular accidents, the drug is used in a volume of 10 ml once a day for 10 days. For toxic and hypoxic encephalopathy, the drug is administered in a volume of 10 ml per injection 2 times a day with an interval of 8–12 hours for 5 days. In case of coma, administer in a volume of 20 ml per 200 ml of glucose solution. For post-anesthesia depression, it is administered once in the same doses. Cytoflavin tablets are taken orally, 2 tablets 2 times a day, 30 minutes before meals, without chewing, at intervals of 8–10 hours, with 100 ml of water. Course duration: 25 days (100 tablets per course). Evening administration of the drug is recommended no later than 18:00. A repeat course is prescribed when the manifestations of cerebrovascular insufficiency increase, but not earlier than 25–30 days after the end of the previous course.
Instructions for use
If the doctor has prescribed treatment with the tablet form of Cytoflavin, take 2 tablets half an hour before meals twice a day. The minimum interval between doses is 8 hours; in the evening you need to take the drug no later than 18 hours. The tablets cannot be chewed; they must be washed down with half a glass of water.
Typically, in this dosage form, the drug is recommended for chronic circulatory disorders; the course of therapy is 25 days. A month after the first course, Cytoflavin therapy can be repeated.
Treatment of certain pathologies using the drug solution is described below:
- Ischemic stroke
. The first dose is administered as soon as possible after the stroke. Place the dropper on a slow setting (60 drops/minute), repeat the therapy twice a day. The dose for people weighing more than 60 kg is 20 ml of Cytoflavin per 400 ml of saline, glucose solution. Patients weighing less than 60 kg are prescribed 10 ml of the drug per 200 ml of solutions.The course is 10 days. For this indication, the drug can be used at any age, even in children.
- Chronic encephalopathies
. The drug is administered intravenously 10 ml once a day with saline (per 100-200 ml), course - 10-14 days. You can then continue treatment with tablets for up to 30 days.
In case of a concussion, 10 ml of the drug is administered twice a day with 200 ml of glucose solution. Course - 7 days or individual.
Side effects of the drug Cytoflavin
With rapid intravenous drip administration, undesirable reactions may occur that do not require discontinuation of the drug: hyperemia of the skin of varying severity, a feeling of heat, bitterness and dry mouth, sore throat. With long-term use in high doses, transient hypoglycemia, hyperuricemia, and exacerbation of gout are possible. Rare adverse reactions include short-term pain and discomfort in the epigastric region and chest area, difficulty breathing, nausea, headache, dizziness, “tingling” in the nose, dysosmia, pallor of the skin of varying severity. Allergic reactions such as itchy skin are also possible.
Efficacy of cytoflavin in spondylogenic radiculomyeloischemia
A. A. Skoromets V. V. Nikitina D. M. Bykovitsky M. L. Pospelova O. G. Sichkar A. P. Skoromets T. A. Skoromets A. V. Solonsky A. A. Timofeeva
The effectiveness of cytoflavin was assessed in the treatment of 60 patients (39 women and 21 men, age 32-64 years) with radiculomyeloischemia of the cervical and lumbosacral localization due to degenerative-dystrophic lesions of the spine. The study design was consistent with a randomized, double-blind, placebo-controlled study in compliance with GCP requirements. For 10 days, 40 patients received cytoflavin intravenously once a day, 20 patients received placebo - 5% glucose solution (control group). Among those receiving Cytoflavin, a significant improvement was observed in 70% of patients with radiculomyeloischemia of the cervical localization and in 65% with radiculomyeloischemia of the lumbosacral segments. In the control group, the positive dynamics of neurological symptoms was 25-30% less than in the main group. Cytoflavin significantly reduced cognitive disorders and improved reparative processes in both central and peripheral neurons. This drug can be recommended for ischemic lesions of spinal cord neurons.
The wide prevalence of spondylogenic neurological disorders and the wide range of their clinical manifestations are well known [1, 4, 6, 7-9, 11]. As for the pathogenesis, irritative-reflex myofascial and muscular-neural, compression and autoimmune-inflammatory radicular and compression-vascular (arterial and venous radiculoischemia and radiculomyeloishemia) syndromes predominate among them. Each of these variants of spondylogenic neurological pathology requires individual pathogenetically based therapy. However, in any variant of the clinical picture of neurological spondylogenic disorders, a vascular - ischemic factor occurs (in a spasmed muscle, a compressed and ischemic nerve at the level of passage through such a muscle - compression-ischemic neuropathy, in a compressed spinal cord root, in segments of the spinal cord).
Therefore, it is almost always necessary to include vasoactive drugs, antihypoxants and antioxidants in the complex treatment of spondylogenic neurological syndromes.
In recent years, NTFF "Polisan" (Russia) has developed a new drug - cytoflavin, consisting of natural metabolites and vitamins. It has an antihypoxic and antioxidant effect, activates the intracellular synthesis of protein and nucleic acids, enzymatic processes of the Krebs cycle, promotes the utilization of glucose, the synthesis and intracellular accumulation of ATP and other macroergs [3].
The purpose of this study is to evaluate the effectiveness of cytoflavin in the treatment of patients with spondylogenic radiculomyeloischemia of the cervical and lumbosacral localization.
Diagnosis was based on the nature of the clinical picture (acute, subacute development), the presence of symptoms of dysfunction of the spinal roots and segmental apparatus of the spinal cord (sensory, motor, vegetative-trophic), as well as its conductors. Degenerative-dystrophic lesions of the spine were determined using spondylography data. The condition of the soft tissue structures of the spine was assessed using MRI data. Patients with cervical radiculomyeloischemia underwent Doppler ultrasound of the vertebral and carotid arteries; 8 patients were able to undergo MRI angiography.
All patients underwent stimulation electroneuromyography and needle electromyography of the extremities. The study was performed using a 4-channel electromyograph Medicor (Hungary) according to a standardized program [2]. The design of the work corresponded to a randomized, double-blind, placebo-controlled study in compliance with the requirements of evidence-based medicine - GCP. The work included 60 patients aged from 32 to 64 years (39 women and 21 men) with a reliable diagnosis of circulatory disorders in the spinal roots and spinal cord without high arterial hypertension and clinical signs of atherosclerosis of the cerebral and aortic vessels.
All studies were carried out comprehensively before and on the 11th day after therapy. Muscle strength was assessed using a 6-point system [10]. The Barthel scale was used to determine the social adaptation index.
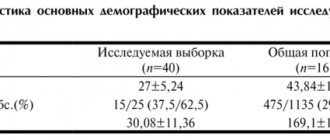
The patients were divided into two groups: the main group - 40 patients who received cytoflavin injections, and the control group - 20 patients who received placebo. Cytoflavin or placebo - 5% glucose solution (10 ml) was dissolved in 200 ml of 5% glucose solution and administered intravenously at a rate of 60 drops per minute once a day for 10 days. Antihypoxants, nootropic and neurometabolic drugs were discontinued 2 weeks before the start of treatment.
Depending on the clinical manifestations, patients were divided into subgroups with localization of spondylogenic ischemia in the cervical segments of the spinal cord (34) and with its localization in the lumbosacral segments (26).
The main complaints in the first of these subgroups were weight loss and weakness of the muscles of the limbs, numbness of the hands, less often headache, dizziness and syncope associated with concomitant circulatory disorders in the vertebrobasilar area. Therefore, it was of interest to study cognitive functions in all patients.
The leading clinical manifestations of radiculomyeloischemia of the cervical segments were motor disorders in the form of flaccid paresis of two or three myotomes or combined tetraparesis (flaccid in the shoulder girdle, central in the lower extremities). Sensitivity disorders manifested themselves as conduction (in 18), segmental or radicular (in 16) disorders. In all patients, vibration sensitivity was reduced by 2-3 times compared to normal. Elements of dynamic and static-locomotor ataxia were identified in 19 patients.
MRI of the cervical spine of 20 patients in this subgroup revealed protrusions of intervertebral discs in 13: C4 - C5 in 2, C5 - C6 in 8, C6 - C7 in 3. Magnetic resonance angiography revealed hypoplasia of one of the vertebral arteries in 6 patients, pathological tortuosity of the vertebral and main arteries - in 2. Spondylography of the cervical spine confirmed the clinically suspected deforming spondyloarthrosis (patients noted a crunch when rotating the cervical spine, limitation of the amplitude of rotational movements and bending in different directions), straightening of the cervical lordosis, the presence of signs of osteochondrosis of the intervertebral discs (sclerosation endplates, decreased height of the intervertebral spaces, calcification of the posterior longitudinal ligament of the spine at the level of the degenerated and prolapsed disc). Kimmerle's anomaly was detected in 3 patients.
Of the 34 patients with radiculomyeloischemia of the cervical localization, in 23 the treatment complex included cytoflavin injections (they belonged to the main group), the remaining patients received placebo (control group).
In 26 patients of the second subgroup, when ischemia was localized in the segments of the lower half of the spinal cord (lower thoracic and lumbosacral), the clinical picture was represented by lower flaccid or mixed paraparesis. Against this background, a more pronounced flaccid paresis of one or two lumbar myotomes was always revealed. Sensitivity disturbances were of a segmental conduction nature with condensation in the most affected dermatome (which corresponded to the radicular type of disorders in radiculomyeloischemia). Half of the patients in this subgroup had impaired function of the pelvic organs sphincters. Signs of vegetative-vascular dystonia in the legs were observed in all patients (marbling of the skin, pastosity, hypothermia, dryness or hyperhidrosis, changes in the trophism of the nails). A significant (2/3 or more from normal) decrease in vibration sensitivity at the ankles indicated venous congestion in the spinal canal and along the posterior surface of the spinal cord with dysfunction of the posterior cords of the latter. Spondylograms of all patients in this subgroup confirmed osteochondrosis of the intervertebral discs (sclerosis of the endplates of the vertebral bodies, decreased height of the intervertebral spaces), smoothness of the lumbar lordosis. MRI revealed protrusions or herniations of intervertebral discs in 18 patients, usually at the level of L4-5 and L5-S1. Of 26 patients with radiculomyeloischemia of the lower half of the spinal cord, 17 received cytoflavin, 9 received placebo.
Data from a neurophysiological study of peripheral nerves and muscles of the limbs in patients with radiculomyeloischemia of the cervical and caudal segments quantitatively objectified their neurological disorders. In all patients, before the start of therapy, an extension of terminal and residual latency, a decrease in the speed of impulses along the nerves, and a decrease in the amplitudes of M-responses during stimulation electroneuromyography of the peripheral nerves of the extremities were recorded.
The dynamics of electrophysiological parameters coincided with the data of clinical status.
When comparing the clinical picture (neurological status) before and on the 11th day from the start of treatment, more pronounced dynamics of motor, sensory functions and the function of the pelvic organs sphincters were noted in patients of the main group (who received Cytoflavin) compared to the placebo group.
Experimental studies of cytoflavin have demonstrated that it promotes the development of reparative processes both in the bodies of neurons themselves and in their processes (conductors in the central and peripheral nervous system). Therefore, it can be assumed that this drug prevents the death of neurons, i.e. promotes their survival during ischemia [5, 12].
When analyzing the results of neuropsychological testing of patients, the absence of significant dynamics in the control group and the presence of cytoflavin were noted (see table).
The table shows that after a course of treatment with Cytoflavin, the performance of neuropsychological testing significantly improves both in patients with circulatory disorders in the cervical segments of the spinal cord and in the vertebrobasilar region (brain stem and posterior parts of the cerebral hemispheres), and with thoracolumbosacral radiculomyeloischemia. This indicates a positive effect of cytoflavin on the brain at any location of ischemia at the level of the spinal cord. Immediate treatment outcomes were assessed as follows.
A significant improvement was considered to be complete restoration of the function of motor, sensory, vegetative-trophic fibers and/or neurons of the spinal cord. The outcome “without dynamics” reflected the absence of changes in the neurological status and data from additional instrumental methods of studying patients. An increase in the degree of dysfunction of motor, sensory, vegetative-trophic fibers and/or neurons of the spinal cord when confirmed clinically and using instrumental research methods was regarded as deterioration. After treatment with cytoflavin (main group), a clear positive dynamics of neurological symptoms was recorded. Significant improvement was observed in 70% of patients with radiculomyeloischemia of the cervical and 65% of lumbosacral segments. A slight improvement was noted in 25 and 30% of patients, respectively. In the placebo group after treatment, the positive dynamics of neurological symptoms was 25-30% less than in the main group.
As for adverse events when administering Cytoflavin, 5 patients experienced a short-term sensation of sore throat, which went away on its own 15-30 minutes after administration of the drug. Thus, the administration of cytoflavin in a dose of 10 ml for 10 days in the acute phase of radiculomyeloischemia reliably restores the functions of both neurons and conductors of the spinal cord, as evidenced by regression of neurological symptoms and positive dynamics of electroneuromyographic parameters. Often observed in spondylogenic radiculomyeloischemia, especially in the cervical localization, impairments in the cognitive functions of the brain are significantly reduced under the influence of cytoflavin. The fact that the cognitive functions of the brain improve under the influence of cytoflavin allows us to recommend it for the treatment of not only ischemic lesions of the spinal cord and spinal roots, but also chronic cerebrovascular insufficiency.
Literature
1. Bogorodinsky D.K., German D.G., Godovanik O.O., Skoromets A.A. Spondylogenic lumbosacral radiculitis. Chisinau: Shtiintsa 1975. 2. Zenkov L.R., Ronkin M.A. Functional diagnosis of nervous diseases: A guide for doctors. M: Medicine 1991. 3. Isakov V.A., Sologub T.V., Kovalenko A.L., Romantsov M.G. Reamberin in the treatment of critical conditions: A guide for doctors. St. Petersburg 2001. 4. Meerson F.Z., Pshennikova M.G. Adaptation to stressful situations and physical activity. M: Medicine 1988. 5. Petrova E.S., Chumasov E.I., Otellin V.A. Morphological assessment of the growth capacity of central nervous system axons in the peripheral nerve. Bull Exp Biol & Med 1998; 2: 233-236. 6. Popelyansky Ya.Yu. Vertebrogenic syndromes of lumbar osteochondrosis. Kazan: Kazan University Publishing House, 1974. 7. Popelyansky Ya.Yu. Diseases of the peripheral nervous system: A guide for doctors. M: Medicine 1989. 8. Skoromets A.A. Ischemic spinal stroke: clinical, anatomical and experimental study: Author's abstract. dis. ...Dr. med. Sci. L 1972. 9. Skoromets A.A., Skoromets T.A., Shumilina A.P. Osteochondrosis of the discs: new views on the pathogenesis of neurological syndromes. Neurol J. 1997; 6:53-55. 10. Skoromets A.A., Skoromets T.A. Topical diagnosis of diseases of the nervous system: A guide for doctors. St. Petersburg: Politekhnika 2002. 11. Skoromets A.A., Skoromets A.P., Skoromets T.A., Thiessen T.P. Spinal angioneurology: A guide for doctors. M: Medpress 2003. 12. Payne JN, Wall PD Munseng Chong Repair of spinal cord disease. Current Opinion in neurology and neurosurgery 1992; 5:4:558-562.
Source Journal of Neurology and Psychiatry named after. S.S. Korsakov No. 5 | 2004
Special instructions for the use of the drug Cytoflavin
Use with caution for nephrolithiasis, gout, hyperuricemia. Can be used during pregnancy (in the absence of allergic reactions to the components of the drug). In critical conditions, the drug should be used after normalization of central hemodynamic parameters. It is possible that blood glucose levels may decrease (which must be taken into account when prescribing), and urine may turn light yellow. In case of hypertension (arterial hypertension), dose adjustment of antihypertensive drugs may be required.
Material and methods
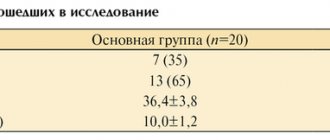
The study included 60 patients, 45 women and 15 men (mean age - 43.4±6.3 years), with stages I and II HE and CVI.
The diagnosis of GE and the stage of the disease were established on the basis of criteria accepted in Russian neurology [24]. The criteria for KVN were: the presence of complaints in patients characteristic of this pathology; the presence of venous pathology in several typical localizations (varicose veins and thrombosis of the veins of the lower extremities, hemorrhoids, varicocele, varicose veins of the esophagus), family “venous” history [4, 6, 17]. The criteria were: the presence of somatic diseases that may cause secondary disorders of venous circulation; severe somatic, mental, endocrine, hematological, oncological, infectious diseases; cerebral stroke in the acute or recovery period up to 1 year; pregnancy, lactation; taking other antioxidant or nootropic drugs within the last 3 months.
Patients were randomized using the envelope method into 2 groups of 30 people. Patients of the main group, 8 men and 22 women (average age - 44.7±3.9 years), received cytoflavin from the 1st to the 25th day of observation, inclusive, 2 tablets 2 times a day against the background of standard basic therapy. Patients in the comparison group, 7 men and 23 women (average age - 44.2 ± 8.5 years), received standard basic therapy: 100 mg of acetylsalicylic acid, individually selected antihypertensive drugs. The control group consisted of 30 practically healthy individuals, comparable to patients by gender and age.
Clinical and instrumental examination of patients was carried out before the start of therapy and over time on the 25th day of treatment. The examination included: general and neurological examination; general and biochemical blood test; ECG; psychometric assessment using scales and questionnaires; Ultrasound examination of cerebral hemodynamics.
For psychometric examination, the following was used: visual analog scale (VAS) - to assess the intensity of the cephalgic syndrome; asthenia scale - to assess the level of asthenic disorders; scale for assessing autonomic disorders; personal questionnaire of the Bekhterev Institute to determine the type of attitude towards the disease; questionnaire SF-36 (Medical Outcomes Study 36-Item Short-Form, MOS SF-36) to study quality of life (QoL). The SF-36 questionnaire consists of 8 scales: physical activity (PF); physical role functioning (RP); physical pain (BP); general health perception (GH) - physical component of health (PCS); vital activity (VT); social functioning (SF); role functioning due to emotional state (RE); mental health (MH) is the psychological component of health (MCS).
The state of cerebral hemodynamics was assessed using an algorithm for complex ultrasound examination (US) of the cerebral vascular system based on the concept of its construction at 5 functional and morphological levels [14]: 1st structural and functional level - common carotid arteries (CCA), internal carotid arteries (VCA), vertebral arteries (VA); Level 2 - middle cerebral artery (MCA); Level 3 - microvasculature (MCR); 4th level - direct sinus (PS); Level 5 - internal jugular veins (IJV), vertebral veins (PV). The study was carried out with a Viamo SSA-640A ultrasound scanner (Japan) using linear sensors with frequencies of 7.5 and 2.5 MHz. The structural characteristics of the vessel were assessed; linear blood flow velocity (LBV) - maximum (Vmax), minimum (Vmin), time-averaged maximum (TAVmax); resistance (IR) and pulsation indices (PI); volumetric blood flow (Vvolmax). To study the MCR, the reactivity of the veins of Rosenthal (VR) was assessed in a test with an orthostatic load on a verticalizer up to an inclination of 60-80°.
Statistical data processing was carried out using the Statistica 8.0 software package. Data are presented as arithmetic mean and standard deviation (M±m). Differences at p<0.05 were accepted as significant.
Drug interactions Cytoflavin
succinic acid, inosine, nicotinamide are compatible with other drugs. Riboflavin: reduces the activity of doxycycline, tetracycline, oxytetracycline, erythromycin and lincomycin. Incompatible with streptomycin. Chlorpromazine, imizine, amitriptyline, by blocking flavin kinase, disrupt the incorporation of riboflavin into flavin adenine mononucleotide and flavin adenine dinucleotide and increase its excretion in the urine. Thyroid hormones accelerate the metabolism of riboflavin. Reduces the severity and prevents the side effects of chloramphenicol (disturbance of hematopoiesis, optic neuritis). Compatible with drugs that stimulate hematopoiesis, antihypoxants, and anabolic steroids.