Testosterone is a hormone produced in the testicles, or more precisely, in Leydig cells. At the same time, in the Sertoli cells, again, which are part of the testicles, the process of sperm formation takes place. Thanks to the coordinated work of these structures, normal sexual and reproductive functions of a man are ensured.
The production of testosterone is controlled by the pituitary gland, a small organ whose dimensions are similar to the size of a pea. Luteinizing hormone (LH) is responsible for the production of testosterone.
The importance of testosterone for the male body
Already in the seventh week of development, testes - gonads - are formed in the male embryo. After two weeks they begin to produce testosterone. When the transition period begins, testosterone levels in the body increase sharply. It is thanks to this that the boy gradually becomes a man. Under the influence of this hormone, the active development of male genital organs and the appearance of secondary sexual characteristics occur, which are characterized by hair growth in the pubic area, body and face.
Thanks to testosterone, protein formation is initiated in various tissues - primarily in muscle. The more of this hormone, the more actively they develop and the stronger they become. In this case, it is difficult not to remember athletes who take anabolic steroids to develop muscles.
Testosterone also affects the normal distribution of fat in the body, the formation and maturation of bone tissue (it is responsible for the timely closure of the bone growth zone). The work of the sebaceous glands is regulated by the amount of the hormone, and it also contributes to the thickening of the vocal cords during puberty, which is expressed in the appearance of a low timbre. In general, testosterone has a direct impact on the appearance and voice a man “gets.”
The list of important functions of testosterone does not end here. It affects almost all body systems, including:
- Cardiovascular. Slows down the processes of atherosclerosis, reduces the manifestations of coronary heart disease, prevents the development of cardiac hypertrophy, and activates the expansion of coronary vessels.
- Central nervous. Affects the ability to navigate in space, memory, attention, speed of thinking, mood (at an increased level it provokes aggressiveness, at a low level it provokes depression). Has an antidepressant effect.
- Urinary . The condition of the prostate gland largely depends on it.
- Hematopoietic . It affects the maturation of red blood cells in the bone marrow.
- And almost the primary function of testosterone is the emergence and maintenance of sexual activity . Due to the fact that it stimulates certain areas of the brain, sexual desire occurs (not only in men, but also in women).
Testosterone also ensures normal erections. It has been verified that under its influence the corpora cavernosa relax and the vessels of the penis are well filled with blood.
WHAT DOES TESTOSTERONE AFFECT?
- Of course, first of all, on the full development of the male reproductive system - the development of the penis and testicles.
- Provides sperm production, sperm formation, ensures male fertility (ability to conceive)
- It affects libido (the very instinct that is responsible for attraction and passion in the male body), and accordingly, affects sexual behavior and sexual activity of a man.
- Development of secondary sexual characteristics in men, such as the growth of a beard and mustache, growth of hair on the chest, abdomen, etc. also occurs under the influence of testosterone.
- Testosterone regulates phosphorus-nitrogen metabolism in the body.
- Plays a big role in ensuring bone density.
- Affects the rate of muscle tissue formation.
- Shapes behavior.
It is obvious that testosterone is very important not only for the physiological functioning of the body, but also for the psychological state of a man. And besides, it determines a man’s behavior (including the degree of aggression, performance, etc.).
I’ll tell you a practical example that very clearly demonstrates how testosterone surges affect a man. One of my patients, shortly before I met him, had his hormones tested. Having received the results and seeing that testosterone was at the lower limit of normal, I decided to correct the situation myself. A smart, educated man - he read it on the Internet, thought about it, bought and used a drug that was previously sold in a pharmacy without a prescription. About a day later I felt a sharp deterioration in my health. He began to have attacks of sweating, chills, lethargy, complete apathy towards life, which was replaced by periodic outbursts of aggression and increased excitability. It should be noted that some injectable testosterone preparations create a depot in muscle tissue and are released gradually over several months. For three months, my future patient could hardly work. By giving the injection, he wanted to improve erectile function, increase vitality and, at the same time, fight excess weight. And as a result, for three months he drove himself into a terrible state.
Therefore, it is important to understand that jokes with hormones are bad.
With normal testosterone levels, a man certainly feels good. What is normal level? The average testosterone level for a man is 12-33 nmol/l (345 – 950 ng/dl).
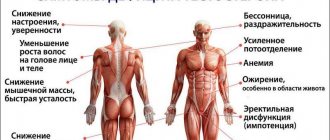
Signs of testosterone deficiency
The importance of testosterone cannot be understated. It affects the condition of the body, and therefore its lack can lead to extremely adverse consequences. You can suspect a hormone deficiency based on the following symptoms:
- deterioration of attention, decrease in concentration;
- decrease or disappearance of libido;
- erection problems;
- increased fatigue;
- decreased strength, decreased muscle mass;
- reduction in the size of the prostate gland and testicles (they acquire a soft consistency);
- hot flashes;
- decreased level of red blood cells, causing anemia;
- brittle bones (osteoporosis);
- infertility caused by a decrease in sperm count.
Also, a decrease in testosterone concentration affects the psycho-emotional state of a man, leading to depressed mood, blues, and depression.
At a recent congress of the American College of Cardiology, research on the use of testosterone for the treatment of age-related androgen deficiency (AAD) was discussed.
Testosterone is a male sex hormone. Secreted by Leydig cells of the testes in men, in small quantities by the ovaries in women and the adrenal cortex in both men and women. Testosterone in men is responsible for virilization and libido, the development of muscle mass. Testosterone also reduces the amount of adipose tissue, increases cell sensitivity to insulin and has a positive effect on lipid metabolism.
Currently, testosterone replacement therapy is used for testicular hypofunction and associated disorders (sexual underdevelopment, functional disorders in the genital area in adolescents, primary eunuchoidism and hypogonadism), as well as for dysfunction of the pituitary gland leading to hypogonadism. In addition, testosterone is used in men suffering from infertility to improve sperm production. Testosterone is also used by some athletes to gain muscle mass and strength.
In recent decades, there has been interest in the possibility of using testosterone drugs to treat age-related androgen deficiency (AAD).)
.
VAD
is accompanied by the appearance of various psychoemotional, vegetative-vascular, metabolic and genitourinary disorders in men.
Symptoms of VAD
include fatigue, decreased libido, depression, hot flashes, and sleep disorders [1]. It should be remembered that each of the symptoms can be caused by other reasons; moreover, according to a number of studies, there is no connection between the level of testosterone in the blood and the presence/severity of symptoms [2]. In 2010, the American Society of Endocrinology released guidelines for the practical use of testosterone [3]. According to the recommendation, only in the presence of symptoms, men should be examined for the presence of VAD, and the diagnosis is made only if a low level of testosterone in the blood is detected twice.
VAD is associated with the fact that testosterone production in the body decreases with age. According to various studies, from 30% to 80% of men over 45 years of age have signs of VAD[4,5]. To compensate for hormonal deficiency, testosterone replacement therapy is used, the main goal of which is to reduce symptoms. According to the studies conducted, it was shown that testosterone increases the amount of muscle mass and reduces the amount of adipose tissue, increases bone mineralization[6] and reduces the level of glycated hemoglobin in patients with diabetes[7]. However, research data on the effect of replacement therapy on mood and quality of life is inconsistent - not all randomized studies have found a positive effect of testosterone therapy on these indicators. [8] There are also conflicting data on the effect of testosterone on erectile dysfunction, although a number of studies have shown a positive effect, an RCT did not confirm the results. [9]
Currently, there are enough Russian publications devoted to the study of the effect of hormone replacement therapy with testosterone in various fields of medicine. The journal Andrology and Genital Surgery (1; 2014) [10] published data assessing the effect of androgen replacement therapy (HRT) on cardiometabolic parameters in men with high cardiovascular risk (CVR) and androgen deficiency. The study involved 52 men aged 30-64 years. It has been shown that HRT with the use of testosterone preparations leads to normalization of testosterone levels, improvement of erectile function, and normalization of basic cardiometabolic parameters.
The problem of the influence of androgens on the cardiovascular system seems quite serious when deciding on replacement therapy in elderly men, since androgen deficiency in itself is not a life-threatening condition for patients (while cardiovascular diseases remain today the leading cause of mortality in developed countries). countries of the world). The most generally accepted point of view of Russian endocrinologists at the moment is that physiological doses of androgenic drugs have a positive or, in extreme cases, a neutral effect on lipid metabolism, without worsening, and possibly improving, the course of cardiovascular diseases in men. [eleven]
In 2014, the FDA began reviewing the safety of testosterone replacement therapy. 2 studies were analyzed. The first study was an observational analysis of patients referred for coronary angiography (CAG) in veterans' hospitals [12]. The work included 8709 men with low testosterone levels (less than 300 ng/dL), the average age of the patients was 63 years, and 80% were diagnosed with coronary artery disease according to coronary angiography. Testosterone replacement therapy was started in 1223 patients an average of 531 days after coronary angiography, with a follow-up period of 27.5 months. According to the study, testosterone use was associated with an increased risk of death, heart attack and ischemic stroke by 29%. The second study was a cohort study of patients (55,593 patients) receiving testosterone replacement therapy. According to the work, the risk of AMI after 3 months of taking the drugs increased by 36% [13].
Given the data on the potential risks associated with the use of testosterone replacement therapy, the FDA has indicated that such therapy is recommended only for men with low testosterone levels due to diseases of the testicles, pituitary gland, or disorders of brain function leading to hypogonadism [14].
Data from one new study and the results of a new meta-analysis on the use of testosterone replacement therapy were presented at the ACC's annual meeting. The first study [15] was an observational study of 7245 men with low testosterone levels. The incidence of the composite endpoint (myocardial infarction, stroke, or death) was 5.5% among those taking testosterone hormone replacement therapy and 6.7% among those not taking it. After adjustment for baseline indicators, there was no statistical difference in the occurrence of cardiovascular complications (CVD). The second study[16], a meta-analysis of 29 studies involving 122,889 men, showed that testosterone replacement therapy does not increase the risk of cardiovascular events. At the same time, the authors identified heterogeneity between studies and in conclusion wrote that to definitively determine the risks of cardiovascular complications in patients taking testosterone, replacement therapy can be done after conducting an RCT.
Links
- Zitzmann M, Faber S, Nieschlag E. Association of specific symptoms and metabolic risks with serum testosterone in older men. J Clin Endocrinol Metab. 2006;91:4335-4343. Abstract
- Berglund LH, Prytz HS, Perski A, Svartberg J. Testosterone levels and psychological health status in men from a general population: the Tromsø study. Aging Male. 2011;14:37-41. Abstract
- Bhasin S, Cunningham GR, Hayes FJ, et al; Task Force, Endocrine Society. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010;95:2536-2559. Abstract
- Trinick TR, Feneley MR, Welford H, Carruthers M. International web survey shows high prevalence of symptomatic testosterone deficiency in men. Aging Male. 2011;14:10-15. Abstract
- Mulligan T, Frick MF, Zuraw QC, Stemhagen A, McWhirter C. Prevalence of hypogonadism in males aged at least 45 years: the HIM study. Int J Clin Pract. 2006;60:762-769. Abstract
- Bassil N. Late-onset hypogonadism. Med Clin North Am. 2011;95:507-523. Abstract
- Jones TH, Arver S, Behre HM, et al. Testosterone replacement in hypogonadal men with type 2 diabetes and/or metabolic syndrome (the TIMES2 study). Diabetes Care. 2011;34:828-837.
- Spitzer M, Basaria S, Travison TG, Davda MN, DeRogatis L, Bhasin S. The effect of testosterone on mood and well-being in men with erectile dysfunction in a randomized, placebo-controlled trial. Andrology. 2013;1:475-482.
- Spitzer M, Basaria S, Travison TG, Davda MN, DeRogatis L, Bhasin S. The effect of testosterone on mood and well-being in men with erectile dysfunction in a randomized, placebo-controlled trial. Andrology. 2013;1:475-482.
- M.N. Mamedov, G.G. Sharvadze, A.A. Evdokimova. The effect of hormone replacement therapy on cardiometabolic parameters in men with high cardiovascular risk and hypogonadism.
- I.I.Dedov, S.Yu.Kalinchenko. Age-related androgen deficiency in men. – M.: Practical Medicine, 2006; 4.2:69-80
- Vigen R, O'Donnell, Baron AE, et al. Association of testosterone therapy with mortality, myocardial infarction, and stroke in men with low testosterone levels. JAMA 2013; 310:1829–1835.
- Finkle WD, Greenland S, Ridgeway GK, et al. Increased risk of nonfatal myocardial infarction following testosterone therapy prescription in men. PLoS One January 29, 2014
- Link to FDA opinion https://tinyurl.com/pqqblva
- Ali Z, Greer DM, Shearer R, et al. Effects of testosterone supplement therapy in men with low testosterone. American College of Cardiology 2015 Scientific Sessions, March 14, 2015, San Diego, CA. Abstract 1126M-13.
- Patel P, Arora B, Molnar J, et al. Effect of testosterone therapy on adverse cardiovascular events among men: A meta-analysis. American College of Cardiology 2015 Scientific Sessions, March 15, 2015, San Diego, CA. Abstract 1195-376.
Authors: Mareev Yu.V., Tsyganova O.B.
Link to news discussion on Medscape: https://www.medscape.com/viewarticle/841098
Why men's testosterone levels may decline as they age
Scientists have found that, starting from about 30 years of age, testosterone levels begin to decline - by about 1-2% annually. By the age of 50-55, and sometimes earlier, testosterone levels can reach only half of the concentration that was in the body at a young age.
Also, the amount of a special protein in the blood gradually increases, which binds sex hormones and thereby reduces the content of biologically active testosterone. This condition is called age-related hypogonadism.
The amount of sex hormone in older age largely depends on a number of genetic factors, as well as diseases of internal organs.
TESTOSTERONE LEVEL DEPENDS ON:
- age of a man: after 25-30 years, hormone production begins to decrease by about 1% per year.
- level of physical activity.
- health conditions (the situation is worsened by various chronic diseases, obesity, diabetes, etc.)
- psychological health - the same notorious stress will negatively affect the production of testosterone.
In addition, the analysis time will also affect the indicators. So, in the morning hours from 4 to 8 am, the maximum concentration of the hormone is observed, in the evening – the minimum. So, when testosterone fluctuates towards a deficiency or excess, a man’s condition worsens. This can happen gradually. So that a man may not even understand what is happening to him and look for the cause anywhere, except in the state of his own hormones.
Diseases that cause testosterone deficiency
It is known that some diseases (acute and chronic), as well as medications taken in combination with age-related changes, can provoke testosterone deficiency. Such diseases include:
- coronary heart disease;
- cirrhosis of the liver;
- obesity;
- arterial hypertension;
- bronchial asthma;
- obstructive pulmonary disease in chronic form;
- diabetes.
In particular, a decrease in testosterone levels causes chronic alcoholism.
The influence of testosterone on the somatic health of men
For a long time, it was generally accepted that testosterone has an adverse effect on the likelihood of development and course of CVD diseases. This point of view was based primarily on the fact that men are more likely to suffer from such diseases. In addition, estrogens, historically considered as androgen antagonists, are known to reduce the risk of cardiovascular events in women. The latter, in particular, is proven by the increase in the number of such diseases after menopause.
In recent years, this position has been subject to serious revision [1]. Methodologically correct studies have not confirmed the relationship between the level of testosterone in the blood and cardiovascular diseases (CVD) in men [2, 3]. Some studies have even shown that higher concentrations of the hormone may have a beneficial effect [4, 5]. Treatment with testosterone drugs is also not accompanied by an increase in the incidence of myocardial infarction, angina or stroke [6, 7], moreover, a decrease in the likelihood of these complications is expected [8, 9]. A number of studies have also shown that the level of testosterone in the blood of men is inversely associated with mortality both from CVD and from all causes in general [10–12].
The nature of the negative effect of decreased testosterone levels on the development of CVD has not been fully established. However, existing data indicate that the adverse effects of hypogonadism on the CVS may be mediated by metabolic syndrome (MS). The latter is a well-known combination of various vascular risk factors, including impaired glucose tolerance, obesity, hypertension and dyslipidemia. The risk of developing MS in patients with hypogonadism is significantly increased [13–15]. These data are so convincing that it has even been suggested that it would be advisable to include hypogonadism among the criteria for diagnosing MS [13]. At the same time, research continues into the questions that arise from these epidemiological data. What is the cause and what is the effect: the components of MS lead to suppression of testicular function or does hypogonadism contribute to their development? What are the mechanisms of these relationships? There is still no clear answer to these questions. It is most likely that there is a bidirectional relationship between hypogonadism and MS.
Insulin resistance (IR), the leading pathophysiological mechanism for the development of MS and its complications, correlates with the level of testosterone in the blood [16]. Patients with hypogonadism are characterized by lower sensitivity to the action of insulin. There is reason to believe that hypogonadism contributes to the development of IR. In particular, signs of resistance to the action of insulin have been identified both in an experimental model of hypogonadism [17] and in men with Klinefelter syndrome [18]. In addition, the development of changes characteristic of MS, including IR, dyslipidemia and obesity, occurs against the background of acute hypogonadism caused by drug therapy [19]. A similar situation occurs, in particular, in the treatment of prostate cancer (PCa) with drugs from the group of gonadotropin-releasing hormone analogues.
The association between hypogonadism and type 2 diabetes mellitus (DM) is also of significant interest. This issue has been studied for quite a long time, and a number of important information has been accumulated, many of which are relevant in the context of the problem under consideration. In particular, men suffering from type 2 diabetes not only more often have low levels of testosterone in the blood [20], but the presence of the latter in healthy men is a prognostic factor for the development of diabetes in them in the future [14]. In addition, the use of testosterone drugs in patients with type 2 diabetes is accompanied by a decrease in the severity of IR and improved control over blood glucose levels [21]. The exact mechanism for the development of these beneficial effects of testosterone has not been established, but the possibility is considered that it is associated with changes in constitution, primarily in the form of a decrease in the volume of adipose tissue.
At the same time, hyperinsulinemia may have a suppressive effect on testicular endocrine function[22]. In addition, it has been shown that suppression of insulin secretion leads to an increase in the concentration of protein that binds sex hormones in the blood [23]. This in turn causes a decrease in the biological activity of testosterone. The suppression of the synthesis of this protein by insulin has been confirmed under experimental conditions [24]. In general, the question of the effect of insulin on testosterone synthesis is still far from being resolved. It can be assumed that various deviations in insulin synthesis can, although in different ways, negatively affect the biological activity of testosterone.
The existence of an inverse relationship between the volume of adipose tissue and the level of testosterone in the blood has been confirmed in many studies [25, 26]. This relationship appears to be complex.
Adipose tissue, and especially its retroperitoneal part, secretes a large number of biologically active substances, which allows a number of researchers to consider it as an independent component of the endocrine system [27, 28]. Many of these substances play an important role in the development of IR, but they can also lead to hypogonadism. In particular, leptin, the secretion of which by adipose tissue is increased in MS, is able to directly suppress the sensitivity of Leydig cells to luteinizing hormone as a result of interaction with specific receptors [29].
Another mechanism of the connection between adipose tissue and testosterone has been known for quite some time and involves the conversion of androgens into estrogens in fat cells as a result of the action of the aromatase enzyme [30]. Thus, adipose tissue can not only suppress the secretion of testosterone, but also reduce its activity, while increasing the concentration of its natural antagonists.
However, the existence of the opposite effect is also assumed. A number of experimental studies have shown that testosterone stimulates lipolysis in fat cells [28], inhibits the entry of lipid molecules into them from the blood [31], and also suppresses the differentiation of stem cells into adipocytes [32]. All these data indicate that blood testosterone levels influence adipose tissue. Confirmation of the validity of assumptions of this kind are the results of clinical studies that have shown the possibility of reducing the volume of adipose tissue in men during treatment with testosterone drugs, which will be discussed below.
Based on the data presented above on the relationship between adipose tissue and testosterone, several theories have been proposed to explain the development of hypogonadism in obese patients (and vice versa). According to one of these theories [33], fat cells convert testosterone into estrogen and also synthesize substances that suppress the function of Leydig cells, leading to the development of hypogonadism. This in turn inhibits lipolysis and stimulates fat cells to take up lipids from the blood, which leads to an increase in the volume of adipose tissue and a further increase in testosterone metabolism. At the same time, due to the increased level of estrogens and adipocytokines, the hypothalamic-pituitary reaction to a decrease in testosterone concentration is inhibited. This hypothesis, in particular, explains the fact that in men with obesity and hypogonadism there is no compensatory increase in the level of luteinizing and follicle-stimulating hormones.
Lipid metabolism disorders, manifested in the form of atherogenic dyslipidemia, also correlate with the level of testosterone in the blood. Moreover, men with hypogonadism tend to have increased levels of total cholesterol (TC) and low-density lipoprotein cholesterol (LDL) [34, 35], while the concentration of high-density lipoprotein (HDL) cholesterol in this group is reduced [36]. These disorders can be corrected by using testosterone drugs. A connection has also been shown between a decrease in the concentration of testosterone in the blood and arterial hypertension [37].
The leading mechanism for the development of CVD is endothelial dysfunction. All of the vascular risk factors described above have a negative effect on the functional state of the endothelium, which leads to the development of atherosclerosis and its complications. At the same time, hypogonadism can directly cause endothelial damage. In an experiment on YL rats. Lu in! a1. found that castration and administration of 5-a-reductase antagonists, which disrupt the conversion of testosterone to its biologically active form dihydrotestosterone, are accompanied by pronounced changes in endothelial cells [38]. On microscopic examination, the endothelial cells were wrinkled, their shape was changed, and intercellular connections were disrupted. In addition, many endothelial cells were covered with red blood cells. In the group of castrated animals, these changes were more pronounced, and they were partially reversed as a result of testosterone administration.
It is also suggested that testosterone and other androgens stimulate the proliferation of endothelial cell precursors in the bone marrow, as well as their release into the bloodstream and connection with areas of endothelial defects. In young men with hypogonadism, a decrease in the concentration of endothelial cell precursors in the blood was noted, while replacement therapy led to a significant increase in these indicators [39]. In addition, the biologically active form of testosterone, dihydrotestosterone, also stimulates the proliferation of vascular endothelial cells themselves. A similar effect of dihydrotestosterone was shown in experiments using bovine aorta [40] and human vessels [41].
Testosterone also affects the release of various para- and autocrine mediators, as well as cytokines, by endothelial cells. In particular, it has been shown that hypogonadism is accompanied by an increase in the level of endothelin-1, which has a pronounced vasoconstrictor effect [42]. Treatment with testosterone preparations was accompanied by a decrease in the concentration of this substance. Testosterone also suppresses the synthesis of many cytokines in the endothelium [43], which have a negative effect on the function of these cells.
Proliferation of vascular smooth muscle cells is an important stage in the development of atherosclerosis. This process is also influenced by the level of androgens in the blood. Testosterone and dihydrotestosterone have an antiproliferative, proapoptotic effect on vascular smooth muscle cells [44, 45], which can provide an antiatherogenic effect.
The data presented above on the influence of androgen levels on the development of MS indicate that, along with a direct effect on the endothelium, testosterone can also exert its influence indirectly through the development of various vascular disorders. The main practical implication of this is the theoretical possibility of eliminating vascular risk factors and, accordingly, preventing or slowing the development of cardiovascular disorders by correcting reduced testosterone levels. A similar effect can be achieved by using testosterone preparations.
For a long time, there were no easy-to-use and effective testosterone preparations, but now a number of new, highly effective drugs have become available, which have significantly expanded the possibilities for correcting testosterone levels. These drugs include various forms of drugs, including oral (limited use), IM, cutaneous, and implantable testosterone-containing pellets.
Testosterone preparations for intramuscular administration are widely used in modern clinical practice. In most cases, they allow the maximum concentration of testosterone in the blood plasma to be achieved within 72 hours after administration. Over the next 10–21 days, testosterone levels progressively decrease. The most commonly used oil solutions are testosterone enanthate and cypionate, which are administered in doses of 200 to 400 mg every 3-4 weeks. [46]. A significant disadvantage of such drugs is the presence of significant fluctuations in the level of testosterone in the blood when they are used. Moreover, in the first days after administration, testosterone levels often significantly exceed physiological values, and in the last days they are inferior to them.
In order to overcome these shortcomings, as well as to achieve a more convenient administration regimen, testosterone undecanoate was created for intramuscular administration. This drug has unique pharmacokinetic characteristics - when used, a stable testosterone level within the physiological range is achieved within 3 days after administration and persists for about 12 weeks. [47]. In this regard, the interval between intramuscular injections of testosterone undecanoate (10–14 weeks or 4 times/year) is almost 5 times greater than that for testosterone enanthate or cypionate (2–3 weeks or 17–26 injections/year) . This feature makes this drug more convenient for long-term replacement therapy.
One ampoule of the drug contains 1000 mg of testosterone undecanoate in 4 ml of castor oil. The contents of the ampoule should be injected very slowly (over about 60 seconds) deep into the gluteal region. After testosterone is administered, undecanoate is gradually released into the blood, where it is broken down by serum esterases to form testosterone. The interval between the 1st and 2nd injections should be 6 weeks, and between subsequent ones - 12 weeks. When using testosterone undecanoate, it is recommended to measure plasma testosterone levels once a year.
Testosterone preparations for cutaneous use include patches and gels. The first patches containing testosterone were proposed in the early 1990s. and were intended for application to the skin of the scrotum. In addition to the inconvenience associated with fixation, the use of such patches is accompanied by an increased level of dihydrotestosterone in the blood, which is explained by the reduction of injected testosterone by 5-a-reductase contained in the skin of the scrotum [48]. Patches for use outside the scrotum do not have this disadvantage, but they often (~32% of cases) cause skin irritation, and 12% of patients develop allergic dermatitis [49]. Gels containing testosterone are less likely to cause skin irritation and allow you to achieve adequate levels of the hormone in the blood. A form for application to the buccal mucosa is also proposed.
Currently, the development of testosterone preparations implanted subcutaneously in the form of granules and microcapsules continues [50]. These drugs have a significant duration of action (up to 6 months), but also have significant disadvantages, the main one of which is the need for surgical interventions during installation and removal.
Testosterone replacement therapy, like any other form of treatment, is associated with the risk of side effects and complications, which determine contraindications to the use of testosterone drugs, as well as the amount of monitoring of patients during such treatment. A traditional concern associated with the use of testosterone drugs is the possibility of an increased risk of developing and/or progression of prostate cancer. In this regard, before starting, as well as periodically during replacement therapy, it is necessary to perform a digital rectal examination and a study of the level of prostate-specific antigen in the blood. It should be noted that more and more evidence is accumulating that normalization of testosterone levels is not accompanied by any noticeable negative effect on the course of prostate cancer [51]. In addition, all men before starting treatment, as well as every 3 months. During the 1st year of therapy and annually thereafter, it is necessary to conduct a study of the hematocrit level. This is due to the fact that testosterone stimulates erythropoiesis, and in some patients a significant increase in the number of red blood cells may be accompanied by a dangerous increase in blood viscosity.
It should be noted that one of the historically prevailing prejudices that limited the use of testosterone drugs was fears of a possible negative effect on the cardiovascular system. However, as we have already indicated above, a better understanding of the true nature of the relationship between the level of testosterone in the blood and vascular risk factors has created the prerequisites for studying the possibility of correcting the latter as a result of testosterone replacement therapy.
The literature widely presents the results of studies of the effect of testosterone preparations on various elements of MS [21, 52–64]. The effect of testosterone preparations on excess adipose tissue has been studied in more detail. A number of studies have shown that hormone replacement therapy leads to an increase in muscle mass and a decrease in fat mass. It should be noted that the reduction in fat mass occurs largely due to the most important, from a clinical point of view, its abdominal part [54].
Thus, in a double-blind randomized study conducted by PJ. Snyder et al., 108 men over the age of 65 years with hypogonadism were treated with a testosterone drug or placebo for 36 months. [55]. At the end of the study, the group receiving testosterone experienced an average decrease in fat mass of 3 kg and an increase in lean body mass of 1.9 kg. There were no significant changes observed among those taking placebo. The possibility of reducing the severity or preventing the development of obesity and other components of MS as a result of the administration of exogenous testosterone has also been confirmed in animal studies [65].
The use of testosterone drugs can also lead to normalization of blood pressure levels. The possibility of such an effect has been shown in studies of obese men with type 2 diabetes [60, 66]. It was noted that the restoration of normal testosterone levels in the blood as a result of replacement
therapy in patients with IR is accompanied by normalization of blood glucose levels [60].
The effect of treatment with testosterone drugs on lipid status is controversial. It has been shown that such treatment may lead to a decrease in HDL cholesterol concentrations, a potentially adverse effect. At the same time, analysis of various fractions of this form of lipoproteins showed that the use of testosterone predominantly reduces the concentration of the 3c form, which is the least important for the antiatherogenic properties of this type of lipoprotein [67, 68]. At the same time, the levels of other fractions, which are much more important, even increased.
Meanwhile, the concentration of LDL cholesterol, which has pronounced atherogenic activity, decreased during testosterone treatment, according to most studies. A decrease in the level of total cholesterol was also noted.
In a study by M. Zitzmann et al. studied the effect of testosterone treatment on blood lipid levels and blood pressure in 66 men with hypogonadism [69]. The treatment led to a significant decrease in LDL levels, as well as systolic and diastolic blood pressure. At the same time, the concentration of HDL cholesterol increased during the treatment period.
We indicated above that hypogonadism can have a negative effect on the endothelium, leading to the development of endothelial dysfunction. The latter, along with hypogonadism, is the leading pathogenetic mechanism for the development of erectile dysfunction and cardiovascular complications in men suffering from MS. These findings, combined with the above data on the beneficial effects of testosterone on CVS, indicate that such treatment may also correct endothelial dysfunction.
This issue has not been studied in sufficient detail to date, but there is some information suggesting that the discussed effects actually take place. In particular, the beneficial effect of treatment with testosterone drugs on certain disorders that play an important role in the development of endothelial dysfunction has been demonstrated. Pharmacotherapy, which led to normalization of testosterone levels in the blood, was accompanied by a decrease in the concentrations of proinflammatory cytokines [70] and endothelin-1 [42], as well as an increase in the concentration of endothelial progenitor cells [71]. These results are very promising and this issue needs further study.
Testosterone preparations can also have a direct beneficial effect on the cardiovascular system. In particular, testosterone has been shown to cause dilation of the coronary arteries. A similar effect has been demonstrated in both experimental [72] and clinical [73] settings. It is believed that this is due to the activation of potassium channels. The possible clinical significance of these findings was demonstrated in a randomized, double-blind study of the effect of testosterone on exercise test performance in men with stable angina pectoris [8]. In the group receiving testosterone, there was an increase in exercise tolerance, which was assessed by changes in the electrocardiogram. The degree of improvement was greater in patients who initially had more severe hormonal disorders. The existence of a similar effect has been confirmed in a number of other works [8, 74–79]. Interestingly, the beneficial effect of testosterone on exertional angina was first described more than 60 years ago [74].
Thus, hypogonadism is an important pathogenetic element in the development of MS and CVD in men. The relationship between a decrease in testosterone levels and vascular risk factors, primarily obesity and IR, is bidirectional, i.e., both groups of disorders mutually aggravate each other, forming a vicious circle. One of the promising ways to correct such disorders is the use of testosterone preparations, currently available in a form convenient for clinical use. All these drugs exert their effect in the same way and contain the same active substance, but the routes of its delivery into the systemic bloodstream and through it to tissues and organs are different. When choosing the most suitable drug for each specific case, many factors should be taken into account, including the individual preferences of the patient.
Medicines that affect testosterone levels
As mentioned earlier, certain medications used in the treatment of certain diseases can lead to a decrease in testosterone concentrations. These medications include:
- used for arterial hypertension - prazosin, reserpine, beta-blockers, clonidine;
- affecting the heart - verapamil, antiarrhythmic drugs, digoxil;
- affecting the gastrointestinal tract - ranitidine, cerucal;
- diuretics – hypotazid, chlorthalidone, veroshpiron;
- affecting the central nervous system - sedatives, antidepressants, amphetamines.
It is unacceptable for a patient to decide to self-prescribe medications. This should be done by a doctor, taking into account the possible negative consequences and impact on sexual function.
How to determine testosterone deficiency
Laboratory testing can determine testosterone levels. To do this, you need to take a blood test in the morning (from 7:00 to 11:00). It is during this period of the day that the hormone reaches its maximum levels. Additionally, an analysis for LH, sex hormone binding protein and a number of other studies are required, which the doctor prescribes on an individual basis. In addition, a specialist is able to suspect a deviation in testosterone production based on clinical signs.
There is also a questionnaire designed for a man to self-assess the level of male sex hormones. He needs to honestly answer a number of questions:
- Is there a decrease in sexual desire, lack of desire to perform sexual acts, or a decrease in pleasure from sexual contact?
- Has growth decreased?
- Has your stamina and physical strength decreased?
- Do you have an irresistible urge to sleep after lunch?
- Do you feel like your enjoyment of life has decreased and that all the best things in life have already passed?
- Has the quality of erections deteriorated?
- Has your performance decreased?
- Has your usual energy and activity decreased?
- Have you become uncharacteristically irritable and/or unexplainedly sad?
- Has your ability to participate in sports become worse recently?
Androgen deficiency is possible if the answers to any three questions or questions 1 and 6 are positive.
Side effects of testosterone
Exogenous administration of testosterone carries certain health risks. Fluoxymesterone and methyltestosterone are synthetic analogues of testosterone. In 2006, it was reported that when women took the drug Estratest, a tablet that is a combination of estrogen and methyltestosterone, the risk of breast cancer increased significantly.
One of the side effects that men complain about is the development of gynecomatia (growth of the mammary glands), but this can be prevented by appropriate selection of a treatment regimen and the use of additional medications.
Another side effect is difficulty urinating.
Use in sports
Athletes use testosterone to improve their performance. There are several methods of administering testosterone, including intramuscular injections, transdermal gels and patches, and implantable capsules.
Anabolic steroids (one of which is testosterone) are used to improve muscle strength and endurance. They make this possible by increasing protein synthesis in muscle tissue. As a result, muscle fibers become larger and recover faster than in normal people. In the 1980s, a series of scandals occurred at the Olympic Games due to improved results, and the use of anabolic steroids was banned by many sports organizations. Testosterone and other anabolic steroids have been designated as a prohibited drug. The level of testosterone used in sports significantly exceeds its doses used for medical purposes for hypogonadism.
These doses are supraphysiological, such testosterone levels are extremely high, which causes many undesirable effects. The use of these drugs is a serious problem, because professional leagues try to hide the use of these drugs.
The issue of steroid abuse has recently come into the spotlight due to the double suicide and murder of Chris Benoit in 2007, but this has not been proven to be the result of steroid exposure as a risk factor.
Changes with aging.
Changes during aging.
As a person ages, testosterone levels gradually decrease. The clinical significance of this phenomenon is currently under debate (andropause). There is some controversy about when older men should be treated with testosterone replacement therapy. The American Andrological Society believes that testosterone therapy should be prescribed when clinical signs suggestive of testosterone deficiency are present. The American Endocrine Association defines hypogonadism as free testosterone levels below minimal values in healthy young subjects.
Previously, age-related decline in testosterone was considered normal.
There is no consensus on testosterone thresholds below which hypogonadism occurs.
Free testosterone (i.e., bioavailable and unbound) or total amount (including the percentage that is chemically bound and unavailable) can be determined. In the US, testosterone levels in men below 300-400 ng/dL in the morning are generally considered low. These findings were independent of age and included older men with low testosterone levels. Therefore, a value of 300ng/dL might be normal for a 65-year-old man, but not normal for a 30-year-old. Signs of testosterone deficiency are nonspecific and can be confused with normal characteristics of aging, such as loss of muscle mass and bone density, decreased physical endurance, and loss of libido.
Replacement therapy can be given by injection, transdermal patches or gels, subcutaneous implants, or oral medications.
Side effects of testosterone therapy include oily skin. Acne, increased hematocrit which may require venipuncture, sleep disturbance and progression of pre-existing prostate cancer.
Exogenous testosterone can suppress spermatogenesis and can lead to infertility. The World Health Organization recommends prostate cancer testing, digital rectal examination and PSA (prostate-specific antigen) before starting therapy, and hematocrit and PSA levels should be monitored during therapy.
Testosterone therapy can prevent or reduce the likelihood of developing osteoporosis, type 2 diabetes, cardiovascular disease, obesity, and depression.
Low testosterone levels increase the risk of developing Alzheimer's disease.
Large-scale studies have not yet been conducted to evaluate the effectiveness and long-term safety of testosterone. Some warn against possible side effects, while others embrace the existing benefits.
How to increase testosterone levels when they are low
Medications prescribed as part of hormone replacement therapy (HRT) can help with this problem. With its help, normal levels of testosterone concentration in the blood are achieved and, thereby, the symptoms of its deficiency are eliminated.
You can undergo all the necessary tests to determine the level of testosterone and other substances related to it in a medical office. A competent urologist-andrologist will prescribe the necessary laboratory tests and interpret their results during the consultation. In case of any violations, an individual drug treatment regimen will be developed for the patient, taking into account indications and contraindications. Only a specialist can prescribe effective therapy that will not cause harm.
Andrologist in Lipetsk: +7 (4742) 90-40-50, and you can also make an appointment online
OVEREXCESS OF TESTOSTERONE
This is a situation where more is not better. For an excess of testosterone also negatively affects the physical and mental state of a man. This is expressed as follows:
- excessive body hair;
- hair loss on the head;
- rash, acne;
- excessively high nervous excitability, outbursts of aggression;
- testicular atrophy, testicular atrophy.
Procedure for elevated testosterone levels: examination, then correction.
Platonov Dmitry Borisovich, Chief Physician of NEON Clinic, Urologist-andrologist.